
STOP “Queer Storytime Adventures for Kids & Families” – to be held in an elementary/middle school library on Sunday May 5th, 2024 at 1:30 pm!
ORIGINAL STORY | UPDATED STORY | GUEST SPEAKERS | VIDEOS | CASS REVIEW OVERVIEW
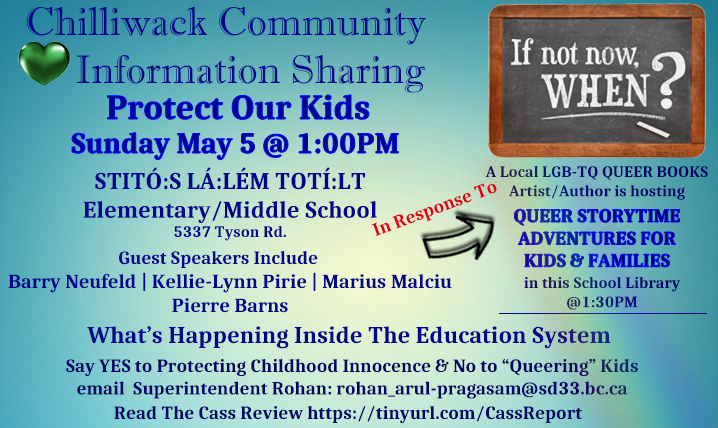
Concerned parents and community members are hosting a Chilliwack Community Information session at STITÓ:S LÁ:LÉM TOTÍ:LT school on Sunday May 5th at 1:00 pm. The address is 5337 Tyson Road, Chilliwack.
Have you, or other parents you know been questioning the socialization and indoctrination that has been happening in our schools, rather than education? Have you heard a little bit about how the Radical-Trans-Queer-Agenda, is being pushed on students of all ages? Would you like to know more about it, and what we can do as a community to stop this?
Educational Guests Speakers Include:
Topics Include:
- School Boards
- What’s Going On In The Education System
- The Cass Review (Independent Review of Gender Identity Services for Children and Young People)
- Pornographic Books In Schools
- No-To-SOGI – Protecting Children
Chilliwack Community Information Sharing is in response to the queering of children, hosted by SD33 in a school library, sponsored by BC UNited Way (Through SD33 Trustee Teri Westerby, also known as: Community Builder Teri).
NOTE:*
The school was contacted, this is not a school sanctioned event. It has nothing to do with the principal or vice principal and they are not happy about it happening . This is a private rental happening at the school on a Sunday afternoon.
It’s the school board and the school district that manage the building rentals during non school hours. You should direct your attention to them. The superintendent is Rohan Arul-Pragasam, his email is rohan_arul@sd33.bc.ca
Hold the SD33 Board and Assistant Superintendents by cc’ing them all.

Willow Reichelt, Chair
604-701-7377
willow_reichelt@sd33.bc.ca
Carin Bondar, Vice Chair
604-997-9978
carin_bondar@sd33.bc.ca
Heather Maahs
604-798-2026
heather_maahs@sd33.bc.ca
Richard Procee
604-702-8409
richard_procee@sd33.bc.ca
Margaret Reid
604-799-5650
margaret_reid@sd33.bc.ca
David Swankey
604-378-4661
david_swankey@sd33.bc.ca
Teri Westerby
778-684-8374
teri_westerby@sd33.bc.ca
Superintendent
Rohan Arul-Pragasam
604-792-1321
rohan_arul-pragasam@sd33.bc.ca
Assistant Superintendent
Kirk Savage
604-703-1714
kirk_savage@sd33.bc.ca
Assistant Superintendent
Paula Jordan
604-703-1725
paula_jordan@sd33.bc.ca
UPDATED STORY
April 29th, 2024, it was reported to RCMP by the people who appear to be the organizers of; and the artist/author of the books that were going to be read at the “Queer Storytime Adventures for Kids & Families” was cancelled, and would be rescheduled. They cited threats of violence as what caused the disruption with this Queer Storytime for Kids.

United Way of B.C. says it wasn’t aware of any ‘threats of violence’ for story time event at Chilliwack school getting axed
CHILLIWACK — Despite assertions by two people that threats of violence were among the reasons for a “Queer Storytime Adventures” event being canceled at a Chilliwack school last week, the United Way of British Columbia said it was not aware of any threats of violence.
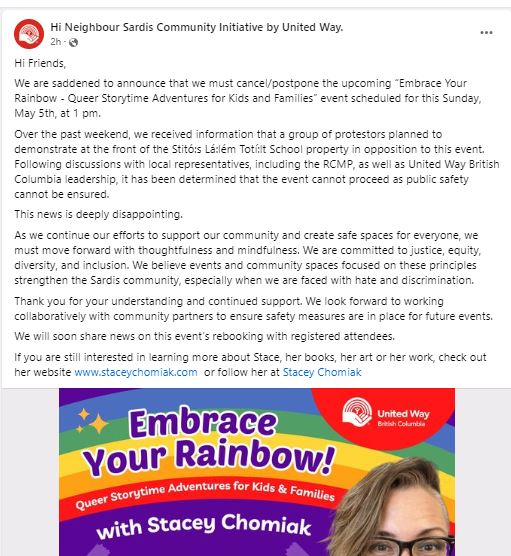
According to a social media post from the Hi Neighbour Sardis Community Initiative by United Way, organizers behind the planned speaking appearance by author Stacey Chomiak said they became aware last weekend that a group of protesters planned to demonstrate at the front of Stitó:s Lá:lém Totí:lt Elementary/Middle School property in opposition to the event, originally scheduled for Sunday, May 5 from 1 p.m. to 3 p.m., leading to its cancellation on school property.
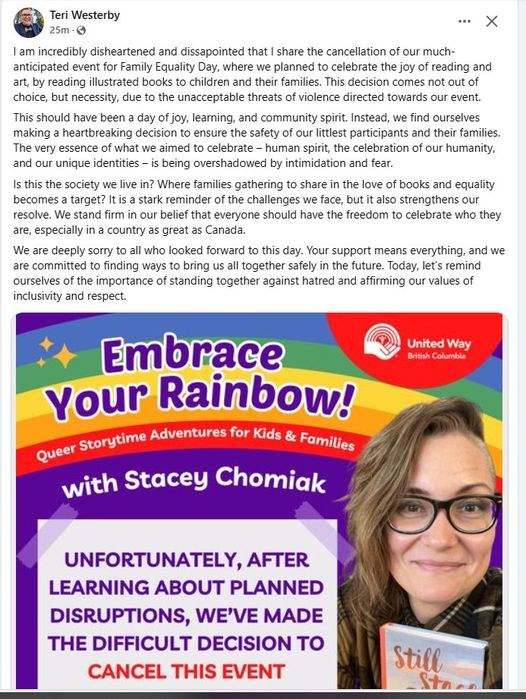
The event was being formally billed as “Embrace Your Rainbow – Queer Storytime Adventures for Kids and Families.”
“Following discussions with local representatives, including the RCMP, as well as United Way British Columbia leadership, it has been determined that the event cannot proceed as public safety cannot be ensured,” Hi Neighbour Sardis Community Initiative by United Way wrote on Facebook.
Chilliwack Board of Education member Teri Westerby wrote on social media that the decision to cancel the event arose “not out of choice, but necessity, due to the unacceptable threats of violence towards our event.” Westerby did not elaborate on social media about what the threats of violence specifically meant or what threats of violence occurred. Chomiak, the author, made a similar statement on Facebook that threats of violence contributed to the event’s demise.
In response to the claims of “violence,” Fraser Valley Today specifically asked United Way B.C. what threats of violence prompted the event to be closed, and whether those involved bomb threats or threats to harm anyone.
A spokesperson for the United Way British Columbia says the cancellation stemmed more from planned protests, not threats of violence.
“United Way B.C. was not aware of any threats of violence, but as we learned protestors were planning a disruption we realized we could no longer ensure a positive experience for everyone involved and made the difficult decision to cancel,” said Dara Hill, United Way B.C. spokesperson. “Our vision is for healthy, caring, inclusive communities.”
Hill added that any comments made by people in their own personal social media feeds did not necessarily reflect the views of United Way B.C.
In response to a media inquiry asking whether there were any threats of violence connected to the event, a Chilliwack RCMP spokesperson told Fraser Valley Today in an email last week that she could not comment on the matter and could only confirm that police were aware of the speaking event.
Fraser Valley Today reached out to Shelley O’Brien, communications manager for the Chilliwack School District, seeking comment on the matter. O’Brien later directed FVT to contact the group behind the event, which in this case was Hi Neighbour Sardis Community Initiative by United Way.
“While the Chilliwack School District offers community rental space at many of our school sites, non-school events such as this one are fully organized and managed by the client renting the facility,” O’Brien wrote in an email to Fraser Valley Today. “Please feel free to reach out directly to the community organization and/or the individual who posted on social media for further information.”
Westerby, who was slated to be the event facilitator, said on social media that he was disheartened by the cancellation.
After learning that threats of violence were not the primary reason for the cancellation, Fraser Valley Today sought comment from Westerby and Chomiak on Friday, May 3 asking what threats of violence occurred that contributed to the event being cancelled. Neither one responded as of Monday afternoon, May 6.
Fraser Valley Today also reached out to the Hi Neighbour United Way group at 5:02 p.m. Thursday, May 2 seeking comment, and was referred to the United Way of B.C. for comment at 2:30 a.m. Friday morning, May 3.
Unfortunately the rented PA system didn’t work. The Guest Speakers were recorded via cell, the volume is quiet. Use headphones, or turn your volume all the way up.
Educational Guests Speakers
The great Transgender COVER-UP is now being EXPOSED! Lawsuits EXPLODING
Gay people are furious that transgender advocacy groups suppressed research showing that puberty blockers and cross-sex hormones are unproven, untested and may hurt and not help trans-identifying children and that most of them will end up perfectly normal gay people, not mutilated trans people. Is this the turning of the tide?
Our Duty Canada’s Official Letter re: The Cass Review
How the Cass Review relates to Canada- an official letter from Our Duty Canada
On the back of the release of the final systematic Cass Review conducted by Dr. Hilary Cass, an accomplished British honorary physician in pediatric disability, ODC crafted an official letter to raise awareness and to call for a similar review in Canada. We sent the letter to public health officials, the Premiere of each province and, of course, our incredibly biased Prime Minister.
We encourage you to use this letter in full or in pieces to send to those in positions of authority who continue to push the now discredited gender affirming care model onto vulnerable children and adolescents.
You can access a PDF copy of the letter HERE or read it below.
We are a group of concerned parents, most of whom have children struggling with gender distress and grappling with the largely unrestricted social and medical options being presented to them in Canada. We believe that no child has the necessary cognitive and psychosocial maturity to provide informed consent to the use of synthetic cross-sex hormones and surgical procedures (referred to as “gender affirming care”) that may permanently damage their health, sexual function and fertility. As a group, we share a very unique perspective based on 2 strengths: (1) We have a wealth of first-hand experience with children experiencing gender distress, because we parent them, as well as with the medical and mental health practitioners who have recommended gender-affirming care for these children, and (2) As dedicated parents, some of whom are also researchers, academics and mental health professionals, we also carefully follow the results of peer-reviewed research in this area, which, to date, has NOT yielded strong evidence of the safety or effectiveness of these gender affirming medical treatments. Therefore, we work to increase public awareness and pressure our social, medical and political organizations to conduct themselves from an evidence-based perspective.
The most recent research-based findings related to gender-affirming care were released on 10 April 2024 in the form of the Cass Review. Given the incredible scope and significance of this review, we are writing to ensure that you are aware of its key findings and corresponding recommendations. Although this systematic review of evidence was executed in England, focusing on The Gender Identity Development Service for children and adolescents which is managed by the Tavistock and Portman NHS Foundation Trust, its findings and recommendations are relevant to the practice of what is referred to as gender affirming care in Canada.
The Independent Review of Gender Identity Services for Children and Young People (The Cass Review) was commissioned by NHS England and NHS Improvement in Autumn 2020 to make recommendations about the services provided by the NHS to children and young people who are questioning their gender identity or experiencing gender incongruence.
Below is a table with several key findings of the Cass Review, the review’s corresponding recommendations, and their relevance to the Canadian context.
| FINDINGS | RECOMMENDATION | RELEVANCE TO CANADA |
| (Page 148) 10.83 The central aim of the assessment process and individualised care plan is to help young people to thrive and achieve their life goals. For the majority of young people, a medical pathway may not be the best way to achieve this. For those young people forwhom a medical pathway is clinically indicated, it is not enough to provide this in the absence of addressing any wider mental health and/or psychosocially challenging problems such as family breakdown, barriers to participation in school life or social activities, bullying andminority stress. | (Page 148) Recommendation 2:Clinicians should apply theassessment framework developedby the Review’s Clinical ExpertGroup, to ensure children/young people referred to NHS gender services receive a holistic assessment of their needs to inform an individualised care plan. This should include screening for neurodevelopmental conditions,including autism spectrum disorder, and a mental health assessment. The framework should be kept under review and evolve to reflect emerging evidence. | The care plan that is applied in Canada to all children who suffer from gender distress is the gender affirming care model. It is based on the unquestioning acceptance of a child’s stated gender identity, no matter their age or individual circumstances, which may include mental health and/or neurodevelopmental conditions. This plan begins with social transition (using the child’s preferred name and pronouns), and, if it is the child’s desire, the care plan then progresses to hormone treatment and surgical interventions.This universal application of gender affirming care to children in Canada is a one-size-fits-all model. This is the antithesis of the individualised assessment and care plan approach recommended in the Cass Review, which is based on the premise that “for the majority of young people, a medical pathway may not be the best way” to help young people thrive and achieve their goals. Moreover, the gender-affirming care model does not allow for the real possibility that children may have mental health and/or neurodevelopmental conditions (comorbidities), or other possible sources of distress that may be plausible causes for their gender-related distress. As is emphasized in the Cass Review, comorbid conditions should always be treated prior to any gender-affirming psychological or medical treatment, because of the significant and irreversible risks that are associated with social transition, cross-sex hormone therapy and body-altering surgeries. Failure to do so not only ignores the fundamental principle to “first do no harm”, but it also increases the risk of liability of mental health and medical bodies and individual practitioners to a rapidly growing population of desisters and detransitioners. |
| (Page 157) 11.43 In summary, there is a lack of evidence about alternative approaches for managinggender-related distress, and it is difficult to obtain information about routine clinical practice or pathways of care for children and young people who do not receive medicalinterventions. An explicit clinical pathway must be developed for non-medical interventions, as well as a research strategy for evaluating their effectiveness. | (Page 157) Recommendation 3:Standard evidence based psychological and psychopharmacological treatmentapproaches should be used tosupport the management of theassociated distress and cooccurringconditions. This should includesupport for parents/carers andsiblings as appropriate. | Assessing patients for mental health and/or neurodevelopmental conditions, and evaluating the possibility that these may be factors contributing to a patient’s gender distress, before considering more invasive and irreversible medical interventions IS NOT, and should never be defined as, “conversion therapy.” Unfortunately, however, Canada’s conversion therapy law (Bill C-4) defines it as such.This has caused mental health professionals to abandon best practice (beginning with less invasive and dangerous interventions before considering more invasive, risky and irreversible interventions) with patients experiencing gender distress, because they are afraid of legal repercussions. There is a growing number of detransitioners and desisters in Canada who sought mental health care under the assumption that they would receive holistic and individualized care, but were treated under the one-size-fits-all gender-affirming care model. Consequently, these patients are now beginning to pursue legal action on the basis of malpractice. |
| (Page 196) 16.34 In considering endocrine interventions, the large number of unknowns regarding therisk/benefits in any one individual and the lack of robust information to help them make decisions present a major problem in obtaining informed consent. | (Page 197) Recommendation 6:The evidence base underpinningmedical and non-medicalinterventions in this clinical area must be improved. Following our earlier recommendation to establish a puberty blocker trial, which has been taken forward by NHS England, we further recommend a full programme of research be established. This should look at the characteristics, interventions and outcomes of every young person presenting to the NHS gender services.• The puberty blocker trial shouldbe part of a programme ofresearch which also evaluatesoutcomes of psychosocialinterventions and masculinising/feminising hormones.• Consent should routinely besought for all children andyoung people for enrolment ina research study with follow-upinto adulthood. | In the absence of robust research findings that demonstrate the safety and effectiveness of puberty blockers, a drug that has such a profound impact on physical and psychological development in children, it is impossible for children or parents to provide their informed consent. Although some argue that the use of puberty blockers (GNrH Analogues) a part of gender- affirming care for children should be banned entirely, Dr. Cass recommends that they only be used in the context of a “puberty blocker trial.” This is certainly a far safer approach than the one we are witnessing in Canada, where Canadian hospitals have given out prescriptions for them over the phone and prior to an initial consultation. |
| (Page 196)16.34 In considering endocrine interventions, the large number of unknowns regarding the risk/benefits in any one individual and the lack of robust information to help them make decisions present a major problem in obtaining informed consent. | (Page 197) Recommendation 8: NHS England should review the policy on masculinising/feminising hormones. The option to provide masculinising/ feminising hormones from age 16 is available, but the Review would recommend extreme caution. There should be a clear clinical rationale for providing hormones at this stage rather than waiting until an individual reaches 18. | Currently there is no requirement for Canadian clinicians to exercise “extreme caution” or “provide a clear clinical rationale” for providing hormones before a child reaches age 18.Establishing these requirements in Canada would go a long way towards protecting children and adolescents who are in very critical stages of physical and psychological growth and who may experience regret once they fully mature. |
| (Page 214) 18.52 Throughout the course of the Review, it has been evident that there has been a failureto reliably collect even the most basic data and information in a consistent and comprehensive manner; data have often not been shared, or have been unavailable. This has led to challenges in understanding the patient cohort, referral data and outcomes, all of which have hindered the work of the Review. More importantly, this has been to the detriment of young people and their families being able to make informed decisions. | (Page 214) Recommendation 16:The National Provider Collaborativeshould coordinate development ofevidence-based information andresources for young people, parentsand carers. Consideration shouldbe given as to whether this shouldbe a centrally hosted NHS onlineresource. | Evidence-based information is not being systematically collected in Canada, and the evidence-based information that is available from research undertaken in other progressive countries is not being made available to children, adolescents and their families when they are being recommended gender affirming care. Countries such as Sweden, Finland, England, Norway and France have produced and/or rely on valuable peer-reviewed research and systematic reviews of evidence when developing best practices in regard to gender-distressed children and adolescents, and these countries are all turning away from the gender affirming care model. Rather than being given the facts, parents in Canada are being asked by medical professionals, sometimes in front of their children, if they would “rather have a trans son or a dead daughter.” This is the suicide myth, and it is an egregious form of emotional blackmail which may to lead to higher rates of suicide ideation if it is presented to children as though it is fact. A recent 20-year Finnish study does NOT show that gender affirming care improves the mental health outcomes of children and adolescents. Perhaps most importantly, this research does NOT find decreased suicide rates in youth who have accessed gender-affirming medical treatment.Gender affirming care, which includes social transition (the use of opposite-sex pronouns, as mandated by Bill C-16, many school district policies, among others), CANNOT be determined as the best course of action in the absence of robust, evidence-based information. |
| (Page 216) 18.66 Without an established research strategyand infrastructure, the outstanding questions will remain unanswered, and the evidence gaps will continue to be filled with opinion and conjecture. | (Page 216) Recommendation 21:To ensure that services are operating to the highest standards of evidence the National Institute for Health and Care Research (NIHR) should commission a living systematic review to inform the evolving clinical approach. | A systematic review of ALL evidence in terms of gender affirming care should be commissioned by Canada’s Ministry of Health and conducted by politically neutral and unbiased research professionals. The review should include all gender clinics, all professionals or organizations recommending or prescribing puberty blockers (GNrH Analogues) or synthetic cross-sex (masculinizing/feminizing) hormones; all hospitals or other establishments performing gender affirming surgeries or procedures; and all organizations providing guidance on, or promoting, gender affirming care. |
| (Page 227) 19.36 The Review has heard that people experiencing regret may be hesitant to engage with the gender services that supported them through their initial transition. Consideration should be given to whether existing service specifications need to be adapted to specifically provide detransition pathways or whether this should be a separately commissioned service.This should be in consultation with people who have been through detransition. | (Page 227) Recommendation 25:NHS England should ensure thereis provision for people consideringdetransition, recognising that theymay not wish to reengage with theservices whose care they werepreviously under. | As we stated above, the number of detransitioners and desisters is rapidly growing in Canada. There are currently no medical or mental health supports in place for detransitioners and desisters outside of the gender affirming care bodies that participated in ultimately harming, not helping, them. Canada’s Ministry of Health must lead the development of support bodies for detransitioners and desisters to avoid further culpability in their ongoing medical harm, neglect and maltreatment on a human rights level. |
| (Page 230) 20.1 The Review recognises that delivery of the aspirations set out in this report willrequire significant changes. The move to the proposed service model will require a phased approach and it may be several years before the full model is operational across the country. Pragmatic strategic and operational plans are required that set out in a transparent way the steps that will be taken to realise the service transformation. This will be essential to build trust and manage expectations. | (Page 230) Recommendation 30:NHS England should establishrobust and comprehensive contractmanagement and audit processesand requirements around thecollection of data for the provisionof these services. These shouldbe adhered to by the providersresponsible for delivering theseservices for children and youngpeople. | Canada currently does not collect any robust data on the outcomes of patients receiving gender affirming care. We do not know how many children are being prescribed puberty blockers and/or cross-sex hormones, or how many are having surgical interventions. We do not know how many of these children have comorbid mental health and/or neurodevelopmental conditions. We do not know the long-term (over 10 years or more) outcomes for this population.This is unconscionable. Without this data, we have no way of knowing what the real risks are to our children. We also have no way of knowing if, and for whom, gender affirming care might be effective. |
It is important to highlight that the Cass Review is not the first significant systematic review to reach the conclusion that there are serious problems with the way gender affirming care has been practiced in several Western countries. Over the past two years, there has been a growing body of evidence confirming that gender affirming care is not evidence-based, and that its experimental nature makes it unsafe and unethical.
A 2023 article in the prestigious British Medical Journal summarizes the findings of other systematic reviews of the evidence that underpins gender affirming care and highlights the serious gaps and weaknesses of this evidence base. The article further states that the “priority for health professionals must be to offer the best possible care to their patients” and that “difficulties arise when the evidence base is preliminary or inconclusive.” The article reminds mental health and medical bodies that, as a fundamental principle of care, they must “ensure that the strength of your management recommendations is in line with the strength of the evidence.”
More recently, in March 2024, the WPATH Files expose and confirm the WPATH’s experimental nature, its lack of proper accreditation, and the knowledge among its members that the gender affirming treatments it continues to recommend are harming children, adolescents and vulnerable adults. The extent of this harm, as WPATH members themselves admit, is unknown at best, and dire at worst.
Also in 2024, this 20-year Finnish study concludes that current research does NOT show that gender-affirming care improves the mental health outcomes of children and adolescents. Perhaps most importantly, this research does NOT find decreased suicide rates in youth who have accessed gender-affirming medical treatment. These research findings are especially important because of the widespread misconception that if trans-identified children and adolescents do not take cross-sex hormones and undergo body-altering surgeries, their mental health will decline and they may even take their own lives. If this were truly the case, there would be ample evidence of these outcomes from around the world. Notwithstanding evidence to the contrary, the suicide myth is an unsubstantiated claim that continues to be made by WPATH and other medical professionals and organizations that recommend gender affirming care.
We urge you to read the final Cass Review and seriously consider its findings and recommendations. In light of this, we once again strongly recommend that a similar review be commissioned in Canada, as has been done in other progressive European countries. Our failure to heed the warnings of those countries that are distancing themselves from the gender affirming care model in favour of less risky and irreversible interventions as a first line of treatment, particularly for children and adolescents, will mean that Canada will continue to fall behind in terms of providing first-rate, evidence-based, individualized, safe and effective medical care to our citizens.
In Support of Children and Families,
Our Duty Canada
Shared from https://ourduty.group/2024/05/01/our-duty-canadas-official-letter-re-the-cass-review/
.