
A British Columbia secondary school is promoting a workshop this week for students between 14-year-olds to 19-year-olds on how to access “gender affirming care,” which includes life-altering surgeries.
As part of its Gender Junction Workshops series, Revelstoke Secondary School will hold a Zoom conference on Feb. 25 advertised to “gender diverse and gender creative youth.”
The workshop will cover a range of topics including “navigating coming out, transitioning and accessing gender affirming care, acquiring gender affirming gear, self advocacy and where to direct your parents, caregivers and teachers for support.”
“Gender affirming care” is a range of interventions designed to affirm a person’s chosen gender identity.
As per BC’s Provincial Health Services Authority, the controversial practice includes medical and surgical procedures such as testosterone or estrogen hormone treatment, vaginoplasty, breast implants, orchiectomy (teste removal) and hysterectomies (uterus removal).
Non-profit organization Trans Connect (ANKORS) coordinator Nicola Hare will be facilitating the workshop for students. The group advocates for more access to “hormones, surgeries, gender-affirming garments, and other trans-positive healthcare options.”
“(We offer) community support groups and events for LGBTQ2IA+ youth and trans, two spirit, intersex, and gender diverse community members of all ages to support togetherness and health,” its website states.

While also serving as a community hub for transgender youth, the website includes a variety of resources on “safe drug use” including a publication titled The Meth Booklet.
One of the sections of the booklet is an explicit guide on how to have “Chemsex” which refers to the use of “drugs to enhance and sustain sexual encounters.”
On Mar. 2. Revelstoke Secondary will also host a similar event designed for parents and family members of “gender diverse youth.”
“You may have a lot of questions about supporting a young person who is gender creative, trans, or questioning. What is the difference between gender identity, expression and sexual orientation?” the event description explains. BC is actively marketing to children
http://www.phsa.ca/transcarebc/child-youth
Shared from https://tnc.news/2023/02/23/bc-workshop-students-trans1/
Fight of our lives to save our kids.
Gays Against Groomers Florida Chapter Leader David Leatherwood addresses the Florida State legislature.
The LGBT community has been hijacked by radical trans terrorists. They use the rainbow as a shield to push their dangerous agenda onto minors. We are sick of being used as their scapegoat.
It’s time to reclaim our community and put an end to the medicalization of minors.
Gays Against Groomers Speaks Out Against Medically Transitioning Kids in Florida
Gender Dissent
The mainstream media either supports gender ideology or remains silent. We at Gender Dissent believe Canadians need to know how society is being altered through policies based on scientifically invalid theories that ignore basic biological and evolutionary reality. And Canadians deserve to know who profits.
ABOUT GENDER DISSENT
We are a concerned group of researchers, writers, parents, professionals and creators coming together from various organizations across Canada. Our aim is to identify and publicize the power and money behind the gender identity industry. We are examining and exposing the powerful corporate and political connections which are reshaping language, laws, institutions and the way we think about being human.
As humans, we are a sexually dimorphic species — there are only two sexes and our sex is observed, not assigned. Since 2017 with the passage of Bill C-16, the Canadian government has denied this biological reality and is now using “gender identity” rather than sex in policy and law. This attempt at social engineering is already creating profits for the medical industry, creating new markets for all manner of surgeries and drugs, as well as creating new marketing constituencies. “LGBT” identities — more accurately “trans” identities — have a purchasing power estimated to be worth $3.6 trillion dollars.
Our educational institutions are teaching children their bodies do not determine their sex and thus preparing young people to adopt medical lifestyles as identity. Our sexed origins are being violated for corporate profits.
Boys and men, whether they try to “feminize” their appearance or not, may now legitimately enter private female spaces, participate in and overwhelm girls and women in their safe spaces and sports.
The mainstream media either supports these developments or remains silent. We at Gender Dissent believe Canadians need to know how society is being altered through policies based on scientifically invalid theories that ignore basic biological and evolutionary reality. And Canadians deserve to know who profits.
Please follow us if you believe that the future of humanity should include and protect biological women and men and foster healthy and intact children.
Wisdom2Action’s Million Dollar Deception
Several youth-focused organizations, including Canadian Gender Report, Detrans Canada and Gender Dysphoria Alliance Canada, pointed out that this law, in practice, will result in the forcible conversion of youth who are same-sex attracted into medicalized, surgically disfigured and sexually dysfunctional “transgender” humans. In effect, Canadian gender doctors are now legally obliged to “trans the gay away” in children who would otherwise mature into healthy gay or lesbian adults (i.e. “convert” them).
READ Full Story Here
Is McKinsey & Company Accelerating Gender Identity Ideology in Canada?
Interestingly enough, starting on July 1, 2023, the Public Service Health Care Plan will start providing $75,000 per lifetime for “gender affirmation.” The benefit is described as “for certain gender affirming procedures not covered by provincial/territorial health plans to help people transition to the gender they identify with, or to remove gender identity all together.”
…a heterosexual man who declares himself to be a woman is considered by McKinsey to be an “LGBTQ+” woman. This is the firm that is receiving millions of dollars from the Government of Canada.
READ Full Story Here
Pushing Gender
SOGI 1 2 3, a program that pushes gender identity ideology in Western Canadian schools, is preparing to expand nationally with the help of a substantial grant from Justin Trudeau’s Liberal government.
SOGI 1 2 3 program, which teaches students from K-12 that they have a sexual orientation and gender identity, is in all 60 British Columbia school districts and six divisions in Alberta.
Under the program’s policies, girls are no longer allowed to have single-sex spaces like washrooms and change rooms. Participation in school sports is also on the basis of self-ID, which means that girls must compete with boys for team spots and podiums.
READ Full Story Here
Shared from https://www.genderdissent.com/
Canadian Women’s Sex-Based Rights
Canadian Women’s Sex-Based Rights – caWsbar – is a cross-Canada, non-partisan coalition of women and male allies working together to preserve the rights and protections of women and girls, as enshrined in the Canadian Charter of Rights and Freedoms (Section 15).
These sex-based Charter rights and protections are currently at risk in Canadian public policy due to confusion between sex and “gender identity or expression” as a result of the passing of Bill C-16 into law in 2017.
We call on all Canadians, regardless of political or religious affiliation, to join us in standing up for women’s and girls’ fundamental sex-based rights to bodily privacy, dignity, fairness and security.
caWsbar is a proud signatory to the Women’s Human Rights Campaign’s Declaration on Women’s Sex-Based Rights along with over 350 international women’s organizations.
Lesbians, by definition, are homosexuals. They are exclusively same-sex – not same-gender – attracted. However, trans rights activists insist that transwomen are women and, therefore, that a transwoman’s penis is a “female penis.” (Here, it should be noted that approximately 80-97% of all transwomen retain their male genitalia.)
Lesbians who object to having transwomen as sexual partners are vilified as “transphobes” and silenced by the very organizations which purport to advocate on their behalf.
READ Full Story Here
The sex of criminals, and victims of crime, are no longer recorded in Canada. Statistics Canada in collaboration with the Canadian Association of Chiefs of Police (CACP) have replaced the variable ‘sex’ with self-declared ‘gender’ in the Uniform Crime Reporting (UCR) Survey.
the government has not publicly announced the removal of “sex” from crime statistics, nor made this information readily accessible to the public. If you want to independently verify this … by contacting Statistics Canada or the CACP. It would also be useful to contact your local police department and inquire as to whether they intend to adhere to this guideline.
READ Full Story Here
BCCNM disciplinary hearing regarding caWsbar founding member Amy Hamm
“This case involves worldviews and rights that have come into conflict, and whether an off-duty nurse is allowed to engage in debate about such a politically charged matter in the public square,” says lawyer Lisa Bildy, co-counsel for Ms. Hamm. “Of course, conflicts are best solved by discussion and debate, not censorship and punishment. The College is tasked with keeping patients safe and regulating the profession in the public interest. But we should be concerned when the regulatory process becomes a tool for use by activists to complain about professionals whose opinions they wish to punish,”
READ Full Story Here
Read our Brief to Parliament regarding Bill C-6 (conversion therapy) and write your MP with your concerns.
Conversion Therapy Bans for Gender Identity: The Harmful Consequences for Women and Girls in Canada. A brief submitted to the Standing Committee on Justice and Human Rights.
Shared from https://www.cawsbar.ca/who-we-are
Documentary Videos
In May of 2021 Sweden announced a change of their policy regarding the medical and surgical transition of children. The change came in the wake of several bombshell documentaries which explored the issue of medicalization of children experiencing gender dysphoria in Sweden and Europe.
The controversial documentary series examined the evidence base of the protocols, the ethics of treating children who cannot consent and the degree of oversight and accountability that clinics held for their patients.
The english speaking world isn’t aware of much of what the documentaries uncovered because of the language barrier, as the films are mostly in Swedish. English captions have been made available and for the first time the films are presented here with english voiceover to make them more accessible.
This transition protocol for children based on “The Dutch Study” had previously been used by clinics in Sweden since around 2014 to start children on puberty blockers leading to cross-sex hormones and surgery.
The “Dutch Study” was originally designed with strict criteria for inclusion which were not being applied to the exploding population of mostly young women who were starting to seek treatment for dysphoria. As such, most patients being put on this “trans train” of affirmation and medicalization were a different population group than those studied in the original Dutch protocol.
As a result, the issues of regret and detransition began to be come more common as people for whom the Dutch Protocol was not designed for started to see that medical and surgical transition did not solve their issues.
When these stories started to leak out, the Swedish investigative journalists at “Mission: Investigate” started talking with regretters and detransitioners and approached the hospitals and clinics who were treating young people at the time to figure out what was going on. Over the next several years subsequent episodes of Mission: Investigate explored other aspects of the modern discourse about the medical treatment of gender dysphoria. The revelations of this series were eventually led to the national health system in Sweden reviewing their protocols and issuing an official policy halting the implementation of the Dutch protocol in treating children with gender dysphoria.
Risking harm from well-intentioned parents and doctors
Despite the absence of supportive evidence, the American Academy of Pediatrics recently suggested that aggressive and clearly harmful medical and surgical interventions might be appropriate for many children who express reservations about their biological sex (Szilagyi 2022; Rafferty et al. 2018).
At the same time, other experts on transgender medicine, including some who are themselves transgender, are raising serious doubts about the quality and value, for young people, of “gender affirming care” (Ault 2021). They are clear that, for youth, the unavoidable short-term harms outweigh the theoretical long-term benefits.
“The latest skirmish was set off by comments made by Marci Bowers, MD, president-elect of the World Professional Association for Transgender Health and Erica Anderson, PhD, president of the U.S. Professional Association for Transgender Health” (Ault 2021).
Dr. Bowers is a skilled gynecologist, who is herself transgender, and performs gender affirming surgery on adults as well as clitoral restoration surgery for adult woman who have suffered genital mutilation (Clitoris.io Undated). Clearly Dr. Bowers does not have a general aversion to major surgery for determined and consenting adults.
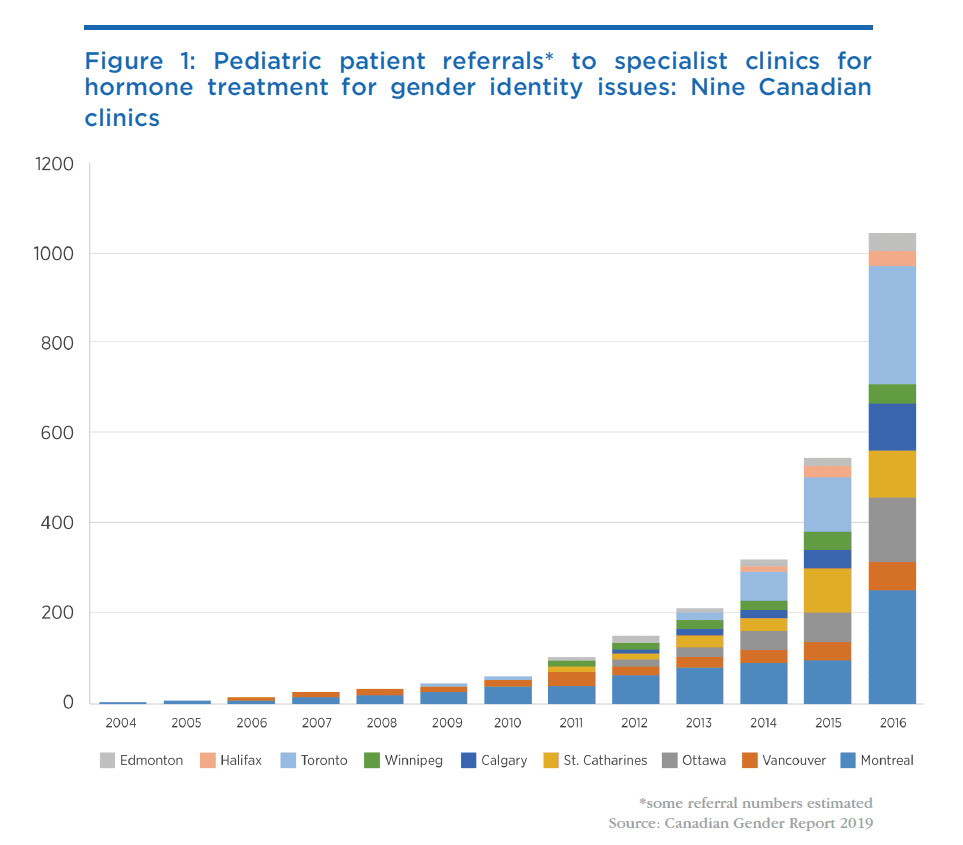
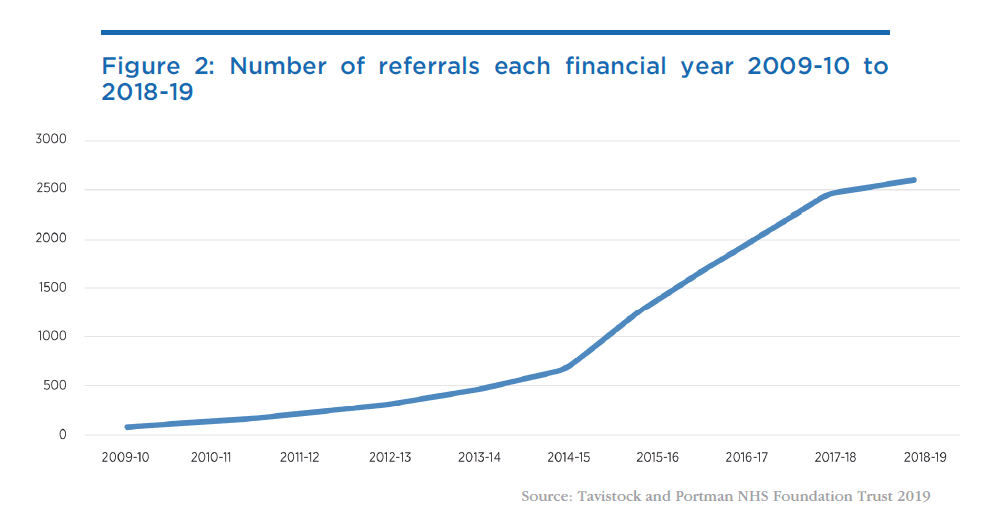
However, Dr. Bowers and transgender psychologist Erica Anderson are distressed and sound an important alarm. They are concerned that children are, on the basis of little or no clinically-proven evidence, being subjected to immediately harmful, complicated, and often irreversible medical and surgical interventions. They note the increasing incidence of, often temporary, rapid onset gender dysphoria (ROGD) where youngsters express an interest in changing from their birth sex, an interest that diminishes or disappears as they get older. Bowers and Anderson emphasize that many people change their minds! And yet at exactly the same time that these alarm bells are being rung, the number of young people now receiving gender affirming care leading to transition is skyrocketing. Figure 1 shows Canadian data and Figure 2 shows data from the UK. Trends are similar in the US (Vesterberg 2022).
Sex reassignment from male to female or female to male is not a benign medical procedure. Hormones and puberty blockers influence growth and development, and trans people are subject to increased risk of various illnesses. A recent Macdonald-Laurier Institute paper (Pike, Hilton and Howe 2021) contains an excellent discussion of the known short- and long-term harms of medical procedures aimed at gender reassignment.
Unfortunately, these aggressive interventions are not based on scientific studies demonstrating overall long-term benefit, nor studies showing which children are most likely to achieve benefit or harm, nor any studies assessing how many young people suffering from ROGD later change their minds and embrace their birth sex. Missing too is information about the proportion of people of various ages who have had gender reassignment procedures who subsequently regret having had those procedures.
Indeed, it seems that mental health issues, and particularly depression, are worse among trans adults (Kattari et al. 2020) than among the general population. There are allegations and opinion, but not sound evidence, that mental health improves after transition surgery (Ring and Malone 2020). We do not know if these mental health disturbances arise because of how trans people are treated by families, physicians, and communities or whether they indicate abnormal biology.
In the absence of the sort of evidence listed above, how can adults, parents, and children decide what to do in the face of conflicting advice from credentialed advisors? And given the politicization of these issues, not least by so-called “conversion therapy” bans, many medical professionals are reluctant to inform young patients fully of risks, or to suggest counselling, for fear of falling afoul of such legislation. Yet medical professionals and regulators should fully expect that detransitioners, those who regret their transition, will be angry and hold to account a medical establishment that refused to inform them fully at the time of their decision about the risks.
In this regard, the experience of the Tavistock Gender Clinic (formally known as the Gender and Identity Development Service (GIDS)) in the UK is instructive. At one time the flagship gender disorder clinic in the UK, the Tavistock has recently been shut down by regulators after a damning independent report (Sex Matters 2022) for precisely these issues: uncritically taking at face value young people’s gender dysphoria and immediately prescribing hormones, “puberty blockers” and even surgery with little or no effort to understand or communicate the risks to their patients. According to The Independent, “Staff, patients and parents have raised concerns that young people using the service were put on the pathway to transitioning too early and before they had been properly assessed.” Massive class-action lawsuits (Lovett 2022) are now expected to be filed against the clinic for failure to respect their professional duties to their patients. One of the lawyers involved, barrister Thomas Goodhead, is quoted as saying that the case “is going to be one of the largest medical negligence scandals of all time” (Times Radio 2022).
The controversies are also emerging in other countries. Vanderbilt University Medical Center, on September 21, 2022, responded to criticisms (Broderick, Davis, Williams, and West 2022) that it profits from and therefore promotes gender transformation in underage youth by announcing that “VUMC requires parental consent to treat a minor patient who is to be seen for issues related to transgender care, and never refuses parental involvement in the care of transgender youth who are under age 18” (Vanderbilt University Medical Center 2022). As a result of the publicity and attention that has been drawn to their activities, VUMC has essentially taken down their website, which critics argue clearly contradicted the clinic’s claims about the safeguards they now claim to apply to transgender care.
Here in Canada, parents of minor children have gone to court to prevent aggressive gender reassignment surgery on a 14-year-old (Graham 2020). Other critics argue that “Canada is too quick to treat gender dysphoria, in minors, with… surgery” (Blackwell 2021). An example is the case of a 16-year-old girl who, while being wheeled into surgery, expressed reservations about the procedure and five years later decided to detransition having decided that despite the double mastectomy she was really a woman (Blackwell 2021).
The problem, as we have noted, is that neither parents, nor clinicians have sufficient research evidence to predict which children will be better or worse off after surgery. And, as previously mentioned in this article, children and adolescents subject to aggressive medical or surgical interventions suffer immediate harms.
At this juncture the very medical professions that should be asking searching questions, and standing up for their members’ responsibility and duty to ensure that their young patients’ interests are fully protected, are trying very hard to suppress discussion of these issues and preventing their members from hearing dissenting views about gender-affirming care (Shrier 2021).
Clinicians are in a quandary: risk the ire of some professional organizations by honestly relating to patients the lack of satisfactory information about the overall benefits and harms of gender transition surgery or put themselves in legal jeopardy when some patients who accepted aggressive therapies suffer and realize that the scientific evidence was insufficient. And for the reasons outlined above, it is difficult for clinicians to predict who will benefit or be harmed by aggressive gender transformation manoeuvres.
Knowing what questions to ask might help
The purposes of health care in general are to improve comfort, function, and life expectancy. And the purpose of mental health services is to influence feelings, thoughts, and behaviour.
What should people with gender dysphoria[1] consider when thinking about complex gender affirming[2] interventions?
First, gender affirming interventions pose immediate and continuing risk to life expectancy and function.
People who transition take supplemental hormones, estrogen or testosterone, which are not compatible with their biological sex. They are exposed to various risks including increased risks of breast cancer for men who take estrogens to transition to woman, and liver disease for men who transition to female. There is also evidence of temporary or even permanent sterility as a result of taking such hormones (National Health Service 2020).
Men who take estrogen for a male to female transition must also take other drugs, like spironolactone, to block the effect of testosterone. Spironolactone interferes with potassium metabolism and increases the risk of blood pressure and heart rate abnormalities, as well as muscle problems. Some transitioners choose to have their testicles removed to take lower doses of estrogen and avoid testosterone blockers. Not everyone responds to hormone disruptors in the same way. The absence of guiding research means it is not clear what measures clinicians should use to decide on the best dose or strategy for each person.
Nor are hormones the only pharmaceutical intervention now raising concerns. The euphemistically named “puberty blockers” – more revealingly described by their correct name, “chemical castrators” – are available in Canada virtually on demand as soon as a minor indicates any interest in gender identity questions. These are not benign drugs but are associated with serious conditions such as early onset osteoporosis (Society for Evidence Based Gender Medicine 2021a). Furthermore, since the use of these drugs as puberty blockers is an off-label use, it is important to understand that no proper clinical trials have been carried out on this use of these drugs. Claims that they are inoffensive and their effects perfectly reversible at any time are not borne out by the information we do have about their effects, especially on young people whose bodies are still in development.
Countries such as Sweden and Finland have recently abandoned uncritical gender-affirming care for minors. According to one Swedish account:
This is a watershed moment, with one of world’s most renowned hospitals calling the “Dutch Protocol” experimental and discontinuing its routine use outside of research settings. According to the ”Dutch Protocol,” which has gained popularity in recent years, gender-dysphoric minors are treated with puberty blockers at age 12 (and in some interpretations, upon reaching Tanner stage 2 of puberty, which in girls can occur at age 8), and cross-sex hormones at the age of 16. This approach, also known as medical “affirmation,” has been endorsed by the WPATH “Standards of Care 7” guideline. (Society for Evidence Based Gender Medicine 2021b)
The experience is similar in Finland, where independent review established the lack of good evidence in favour of gender affirming care:
A year ago, the Finnish Health Authority (PALKO/COHERE) deviated from WPATH’s “Standards of Care 7,” by issuing new guidelines that state that psychotherapy, rather than puberty blockers and cross-sex hormones, should be the first-line treatment for gender-dysphoric youth. This change occurred following a systematic evidence review, which found the body of evidence for pediatric transition inconclusive.
Although pediatric medical transition is still allowed in Finland, the guidelines urge caution given the unclear nature of the benefits of these interventions, largely reserving puberty blocker and cross-sex hormones for minors with early-childhood onset of gender dysphoria and no co-occurring mental health conditions. Surgery is not offered to those [under] 18. (Society for Evidence Based Gender Medicine 2021c)
Second, transitions do not necessarily lead to better lives. Walt Heyer, a former transgender female wrote:
The reprieve I experienced through surgery was only temporary. Hidden underneath the makeup and female clothing was the little boy hurt by childhood trauma. I was once again experiencing gender dysphoria, but this time I felt like a male inside a body refashioned to look like a woman. I was living my dream, but still I was deeply suicidal. (Heyer 2019)
Imagine his resentment if his parents had encouraged doctors to do his transition before he had matured.
People considering transition should be asking tough questions about the proportion of people who benefit or are harmed from such transitions and medical practitioners have a professional duty to make their patients aware of these risks. Sadly, for youngsters such research has not been done, partly because the number of candidates for transition treatments is low and it is difficult to do an appropriate trial.
Curiously, outside the area of gender affirming care, physicians and regulators are themselves cautious and ambivalent about the use of even insignificant amounts of hormones to influence function and appearance.
Men wishing to take tiny amounts of anabolic steroids like testosterone to improve their appearance or athletic performance will have difficulty obtaining steroids from a doctor. Indeed, they might be forced to buy the drugs at their local gym or from a street vendor. The reason is that the medical establishment feels that even low doses of testosterone used for body sculpting might be harmful.
Women asking for estrogens are warned about the increased risk of some cancers and of cardiovascular disease.
The risk of harm from hormone therapy is the same whether the drug is obtained from street vendors, physicians, or pharmacists.
Do some adults benefit?
Some people believe, as adults, they might be happier if they were not their birth sex. Bruce Jenner, the male Olympic athlete, who became the female actor Caitlyn Jenner, is one example and Chaz Bono, formerly Chastity Bono, transitioned from female to male. Fully informed adults under the care of competent professionals are entitled to make such choices and may feel the benefits outweigh the risks, although here again we lack the medical research and data to inform them properly about the consequences of these choices.
Conclusion
Motivated and consenting adults should have the freedom to choose how to live their lives. If clinicians are prepared to offer drug and surgical treatments for gender transition, patients should be free to have them. The regulators’ and lawyers’ responsibility is to evaluate whether clinicians gave the patients, who subsequently changed their mind, the information they needed to make an informed choice. If regulators agree with this rationale then people should be free to ask for and receive other drugs that they believe will improve their experiences, thoughts, feelings, and behaviour including hormones to modify appearance, and drugs, uppers, and downers, such as amphetamines or valium to alter their mood.
Adults and the parents of young children who want to change birth sex face a quandary. Doctors are free to opine on any topic, and many people blindly accept medical advice and recommendations. Most medical suggestions are based in science. Sometimes when science is insufficient, they are based on art. Advice about gender transition for youngsters is one example of such art too often masquerading as science.
When clinicians, making artful suggestions and constrained by conversion therapy bans not to communicate their complete thoughts, offer different and even contradictory conclusions, patients and parents are forced to choose between their opinions and must recognize that majority opinion does not rule. Historically doctors believed that many unscientific treatments were valuable. George Washington had bloodletting for a sore throat and died of anemia, others had radiation therapy for thyroid disease and died from cancer. Sadly, the list of harmful treatments that were widely accepted is not short.
In the face of evidence that some people change their minds, and the clear immediate harms from transition treatments, parents and doctors would be well-advised to support and respect children who claim they are a different gender from the one they were born with, understanding that that does not simply mean acquiescing uncritically in every demand for immediate transition. Professionals and parents should also be clear that some, but not all, people regret invasive and permanent transition treatments and should be advised that proxies (like parents) cannot make such decisions and that the child should wait until adulthood to consider transition and to get information that is current when they decide to explore transitioning.
About the author
David Zitner is a retired family physician, former Professor in the Dalhousie University Faculties of Medicine and Computer Science and the founding director of the graduate program in Health Informatics. He has contributed to the boards and advisory committees of a several Canadian health organizations, including the Canadian Medical Association and accreditation Canada. He has chaired the quality, utilization and other committees of the Halifax Infirmary, a major Canadian teaching hospital. He has published in the popular press and in peer reviewed medical journals and was co-author of the Atlantic Institute for Market Studies Fisher prize winning papers “Operating in the Dark” and “Public Health: State Secret.”
See sources, read more, shared from https://macdonaldlaurier.ca/gender-dysphoria-in-children-risking-harm-from-well-intentioned-parents-and-doctors/
I Thought I Was Saving Trans Kids. Now I’m Blowing the Whistle
There are more than 100 pediatric gender clinics across the U.S. I worked at one. What’s happening to children is morally and medically appalling.
By Jamie Reed February 9, 2023
I am a 42-year-old St. Louis native, a queer woman, and politically to the left of Bernie Sanders. My worldview has deeply shaped my career. I have spent my professional life providing counseling to vulnerable populations: children in foster care, sexual minorities, the poor.
For almost four years, I worked at The Washington University School of Medicine Division of Infectious Diseases with teens and young adults who were HIV positive. Many of them were trans or otherwise gender nonconforming, and I could relate: Through childhood and adolescence, I did a lot of gender questioning myself. I’m now married to a transman, and together we are raising my two biological children from a previous marriage and three foster children we hope to adopt.
All that led me to a job in 2018 as a case manager at The Washington University Transgender Center at St. Louis Children’s Hospital, which had been established a year earlier.
The center’s working assumption was that the earlier you treat kids with gender dysphoria, the more anguish you can prevent later on. This premise was shared by the center’s doctors and therapists. Given their expertise, I assumed that abundant evidence backed this consensus.
During the four years I worked at the clinic as a case manager—I was responsible for patient intake and oversight—around a thousand distressed young people came through our doors. The majority of them received hormone prescriptions that can have life-altering consequences—including sterility.
I left the clinic in November of last year because I could no longer participate in what was happening there. By the time I departed, I was certain that the way the American medical system is treating these patients is the opposite of the promise we make to “do no harm.” Instead, we are permanently harming the vulnerable patients in our care.
Today I am speaking out. I am doing so knowing how toxic the public conversation is around this highly contentious issue—and the ways that my testimony might be misused. I am doing so knowing that I am putting myself at serious personal and professional risk.
Almost everyone in my life advised me to keep my head down. But I cannot in good conscience do so. Because what is happening to scores of children is far more important than my comfort. And what is happening to them is morally and medically appalling.

The Floodgates Open
Soon after my arrival at the Transgender Center, I was struck by the lack of formal protocols for treatment. The center’s physician co-directors were essentially the sole authority.
At first, the patient population was tipped toward what used to be the “traditional” instance of a child with gender dysphoria: a boy, often quite young, who wanted to present as—who wanted to be—a girl.
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
This concerned me, but didn’t feel I was in the position to sound some kind of alarm back then. There was a team of about eight of us, and only one other person brought up the kinds of questions I had. Anyone who raised doubts ran the risk of being called a transphobe.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
That’s all it took.
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
Side Effects
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”
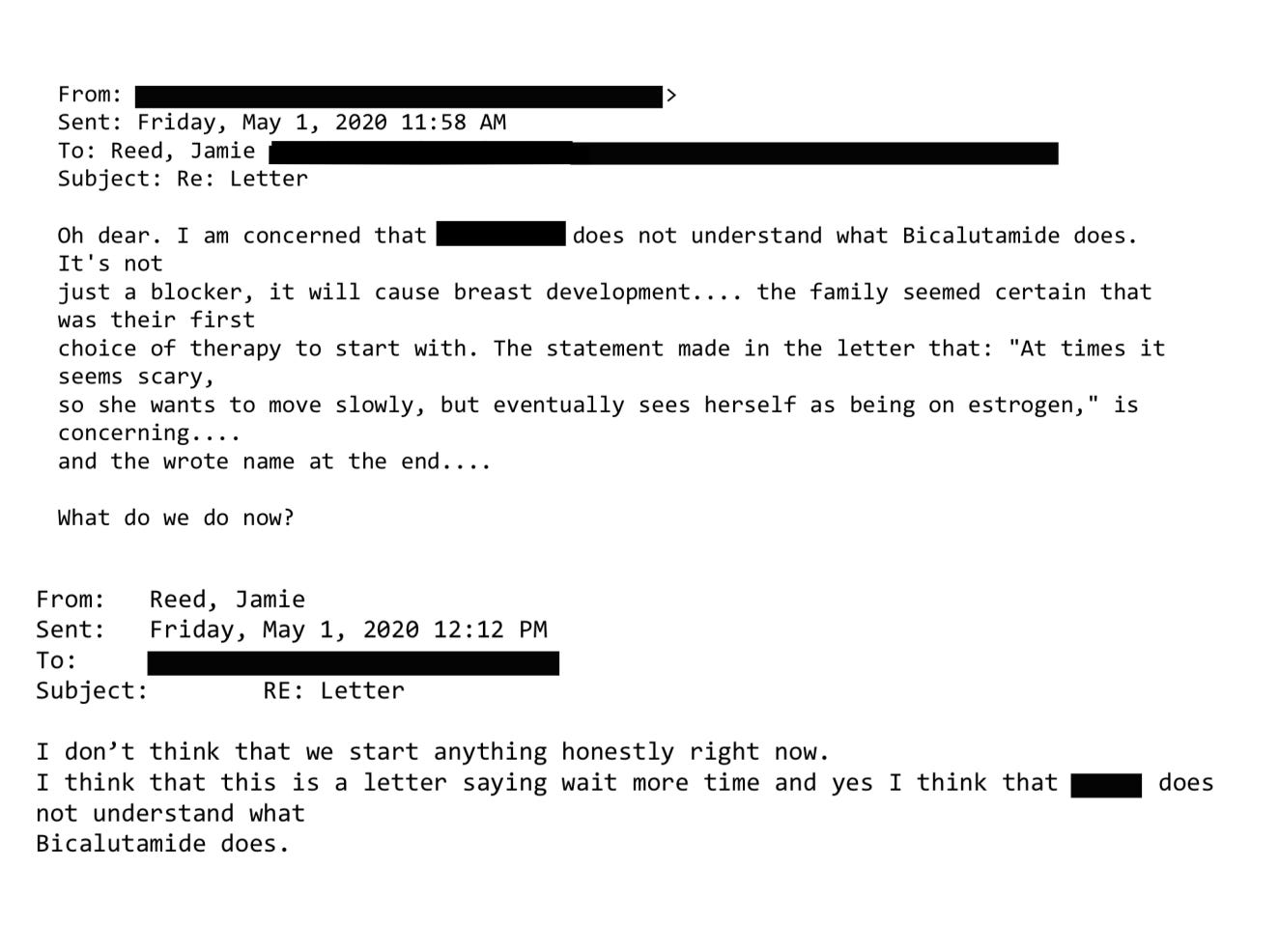
Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—-affects the rest of the body. I doubt that any parent who’s ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:

Neglected and Mentally Ill Patients
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
Some weeks it felt as though almost our entire caseload was nothing but disturbed young people.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
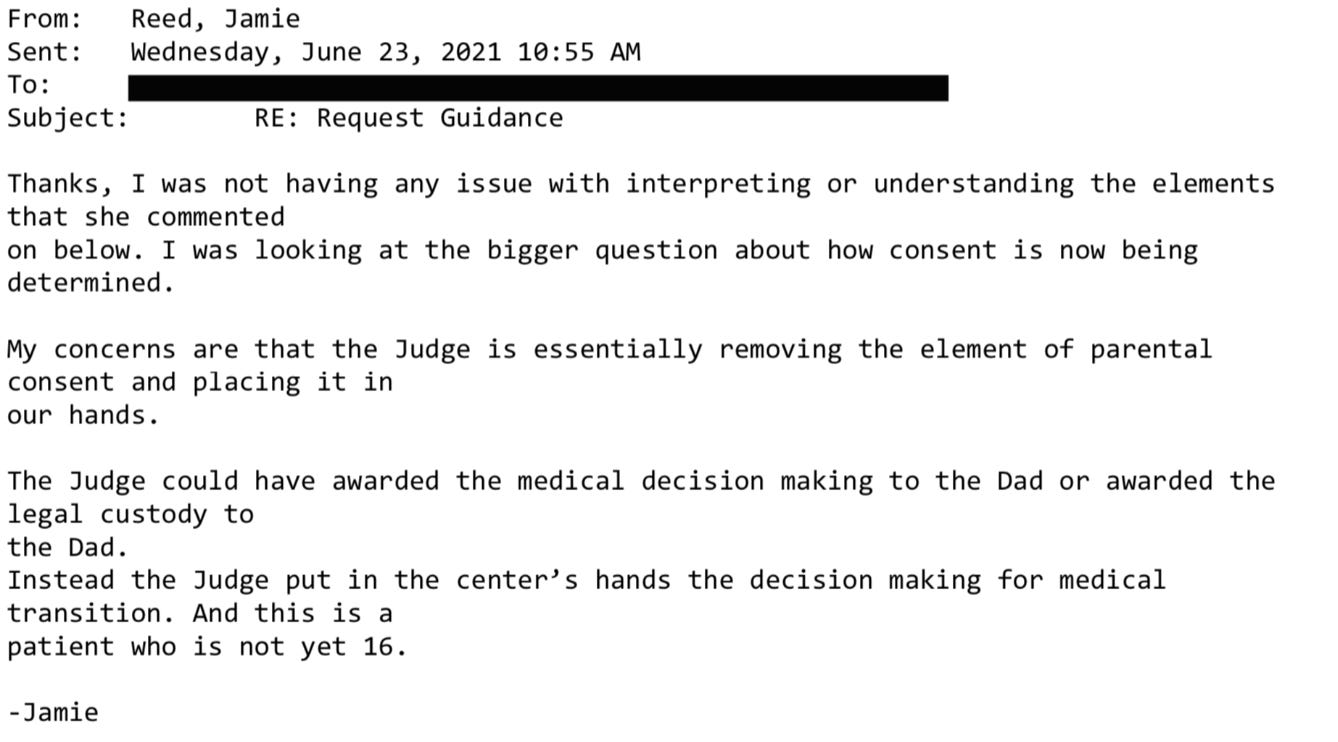
In Loco Parentis
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
The father adamantly disagreed, said this was all coming from the mother, and a custody battle ensued. After the hearing where our doctor testified in favor of transition, the judge sided with the mother.
‘I Want My Breasts Back’
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
But we created a document anyway and called it the Red Flag list. It was an Excel spreadsheet that tracked the kind of patients that kept my colleague and me up at night.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
‘Get On Board, Or Get Out’
My concerns about what was going on at the center started to overtake my life. By spring 2020, I felt a medical and moral obligation to do something. So I spoke up in the office, and sent plenty of emails.
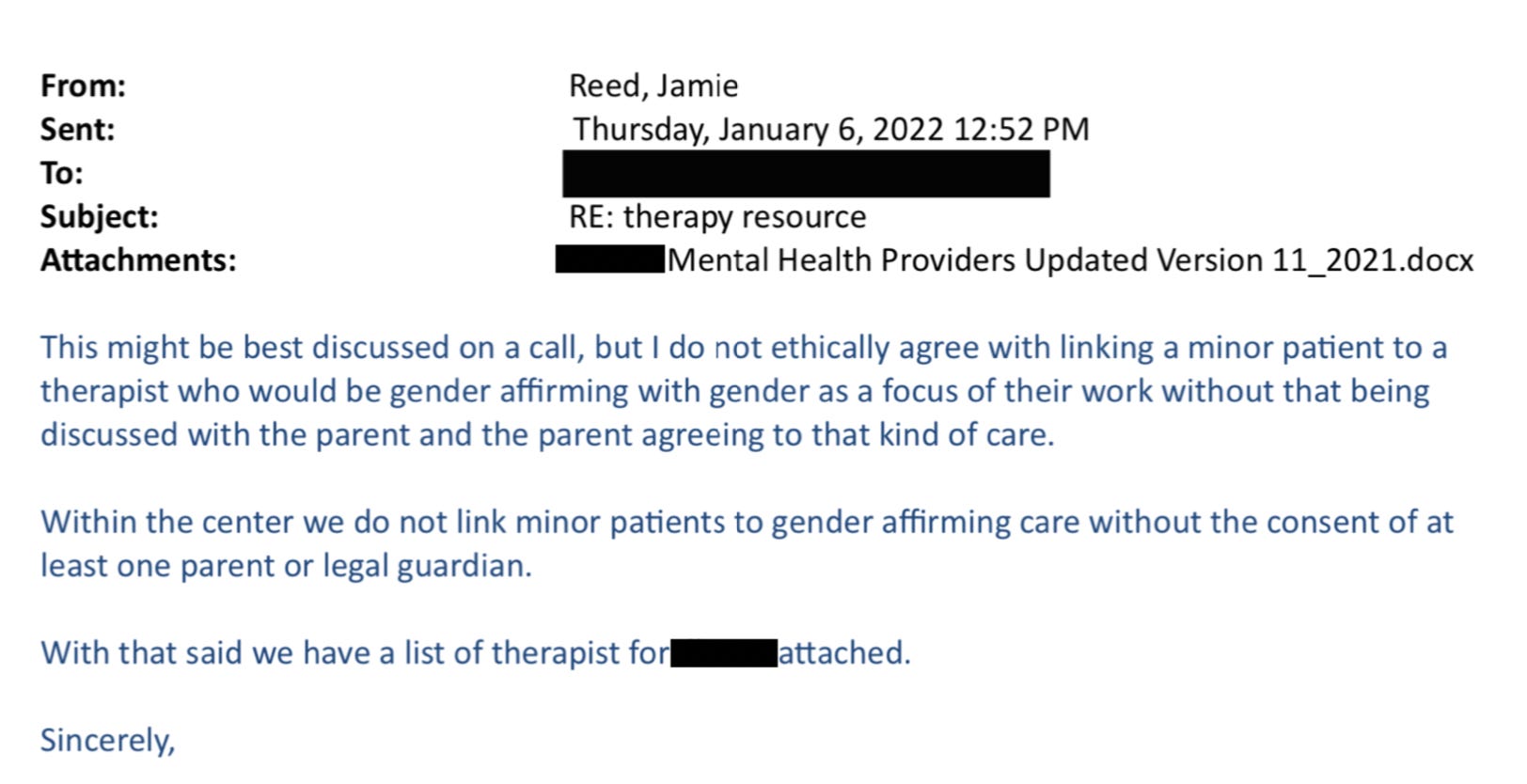
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”
In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.

What I Want to See Happen
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Click here to read Jamie Reed’s letter to the Missouri AG.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
Some critics describe the kind of treatment offered at places like the Transgender Center where I worked as a kind of national experiment. But that’s wrong.
Experiments are supposed to be carefully designed. Hypotheses are supposed to be tested ethically. The doctors I worked alongside at the Transgender Center said frequently about the treatment of our patients: “We are building the plane while we are flying it.” No one should be a passenger on that kind of aircraft.
Shared from https://www.thefp.com/p/i-thought-i-was-saving-trans-kids
Detransitioned Ontario woman sues doctors who removed her breasts, uterus
‘Acknowledging that I cannot bear my own children has been devastating. Some days, the pain of what I’ve done to myself is overwhelming. I cry and I can’t stop.’
Wed Feb 22, 2023 – 12:36 pm EST
ORILLIA, Ontario (LifeSiteNews) — A Canadian woman who regrets her so-called “gender-reassignment surgeries” is now suing the medical professionals involved in her “transitioning” process.
34-year-old Michelle Zacchigna from Orillia, Ontario, who underwent hormone treatment and surgeries more than a decade ago in order to appear as a male, has launched the very first Canadian de-transitioner lawsuit, suing the eight doctors and “mental health experts” who saw her through the self-mutilation process.
“I’ve been holding this card close to my chest for a while, and I’m ready to show it,” Zacchinga tweeted on Tuesday. “In November 2022, I commenced legal action against the Canadian health care providers that facilitated my medical transition in Ontario.”
I’ve been holding this card close to my chest for a while, and I’m ready to show it. In November 2022, I commenced legal action against the Canadian health care providers that facilitated my medical transition in Ontario.
— Michelle🦎♀ (@somenuancepls) February 21, 2023
“I will live the rest of my life without breasts, with a deepened voice and male-pattern balding, and without the ability to get pregnant,” she said.
“Removing my completely healthy uterus is my greatest regret,” Zacchigna lamented.
In a statement, Zacchigna explained that she first thought about transitioning back in 2009 when she was just 21 years old. Depressed, anxious, and self-harming, she found a community online where she finally felt at home.
“Online, I was sucked into a world where it felt like I was finally somewhere I belonged,” she recalled. “In places like Tumblr, there was constant reassurance that only trans people spend so much time thinking about their gender (not actually true) and that every trans person has doubts about transitioning.”
Zacchinga began the process of “transitioning” in 2010, saying that she had never experienced gender dysphoria beforehand. She was told that this was normal, and that many discover their true identities later in their lives. She was allowed to self-diagnose, and less than one year after she had “come out to herself,” as she described it, she had already been placed on synthetic testosterone which permanently altered her voice and appearance.
Just fourteen months later, she underwent a bilateral mastectomy to remove both her breasts.
8 years into her transition, Zacchinga also had her uterus removed, which was fully covered by taxpayers through the Ontario Health Insurance Plan (OHIP).
“Acknowledging that I cannot bear my own children has been devastating. Some days, the pain of what I’ve done to myself is overwhelming. I cry and I can’t stop. Other days, I’m angry that I wasn’t screened for the diagnoses I later received before I was prescribed hormones.”
Years into treatment, Zacchingna was diagnosed with ADHD, tic disorder, borderline personality disorder, anxiety disorders, autism spectrum disorder and traits of PTSD – all of which Zacchingna says the doctors never investigated, just as they never challenged or contradicted her request to transition.
According to the legal filing, “Zacchigna alleges that all the defendants failed to address her serious mental health issues and developmental disabilities and instead only offered her irreversible medical interventions. She alleges that her desire to become transgender was never challenged, and alternative treatment options were never offered.”
“The defendants permitted Michelle to self-diagnose as transgender and prescribe her own treatment without providing a differential diagnosis or proposing alternative treatments,” reads the claim.
Now, more than a decade after she began the “transitioning” process, Zacchinga has taken the route of advocacy in the hopes of sparing other vulnerable young people from making the same horrible decision, explaining that her advocacy is not just for herself, but that she is hoping by her actions to be able to “raise awareness of the recklessness of ‘gender-affirming healthcare.’”
“My advocacy is largely not for me,” she said. “What happened to me cannot be undone. But rather, it is in hopes of preventing it from happening to someone else.”
Shared from https://www.lifesitenews.com/news/detransitioned-ontario-woman-sues-doctors-who-removed-her-breasts-uterus/