
SARS-COV-2 Antibody Testing Explained.
Dr Steven Pelech Ph.D. President & Chief Scientific Officer at Kinexus Bioinformatics speaks at the Idaho Victims of Pandemic Policy & Law about the Kinexus SARS-COV-2 Antibody Testing Clinical Study. People with antibodies continually being exposed to the virus are naturally boosted by those exposures.
Growing evidence that people that have had COVID-19 prior to triple vaccination have poorer outcomes and more severe vaccine injury. Vaccination against COVID-19 in those previously with COVID-19 may actually reduce natural immunity.
Antibody dependence Enhancement is where the virus is coated with the antibody and stick to the immune cells and gains entry to those immune cells and wipe them out. Repeated vaccinations will confuse your immune system.
Clip taken from EpochTV Live – Sep 26,2022 – Victims of Pandemic Policy & Law Panel Discussion
https://www.theepochtimes.com/victims-of-pandemic-policy-law_4753445.html
(need to be a paid member to watch the full version)
[Webmaster Comment]
I have given blood for Dr. Pelech’s SARS-CoV-2 Antibody study.
If you are interested in participating fill out the form here https://forms.gle/jk3t547gSJDre1aAA
I tested many people in my family, including adults ages 57 to 89, and children from ages 7-18. I’m sharing my communication that I had with Dr. Pelech, before we decided to join his study, including:
My own antibody results (vaccine-free and naturally immune).
Results from my mother, (vaccinated and naturally immune).
Other communications. Dr. Pelech said I could share anything he sent me.
Read Here.
Dr. Steven Pelech first response to me, after I contacted him in January, 2021
My SARS-CoV-2 Antibody Results
Results of an elderly woman who was naturally immune, and vaccinated.
View one of Dr. Steven Pelech’s peer reviewed studies https://peoplesworldwar.com/adults-show-preexisting-antibodies/
Original antigenic sin. Molecular mimicry. Apoptosis. What do these scientific terms, COVID and vaccines have in common? Join Jessica Rose, Ph.D. and Steven Pelech, Ph.D. for an intriguing conversation on today’s ‘Good Morning CHD’ as they deep-dive into this often censored topic. What they share with viewers is critical.
Another similar interview here too:
https://live.childrenshealthdefense.org/chd-tv/shows/an-informed-life-radio-with-bernadette-pajer/its-all-about-that-spike-with-jessica-rose-phd–steven-pelech-phd/
Klahowya everyone, (Written in April 2022)
Some of you have contacted me about the recent CTV and Globe news tories about an extra-ordinarily poor scientific paper and its erroneous conclusions that was drafted by Dr. David Fisman, one of his colleague and a graduate student. We discussed the many deficiencies of this publication at the Canadian Covid Care Alliance Scientific and Medical Advisory Committee meeting this evening, and we will be preparing a more in-depth critique of this article in the coming days. One of our Committee members, Dr. Byram Bridge has already produced an opinion piece, which I am sharing with you below.
In addition, members of our Committee wrote a scientific publication that was accepted today for publication in a peer-reviewed journal. McLeod, D., Martins, I., Pelech, S., Beck, C., Shaw. C.A. (2022) Dispelling the myth of a pandemic of the unvaccinated. Int. J. Vaccine Theory Practice Res. (in press). I have attached a copy of the pre-print of this article. Even though the manuscript was written over a month ago, it further explains why the Fisman publications is so wrong in its pronouncement that COVID-19 is being driven by the vaccinated.
🙂 Best wishes from Steven Pelech.
Attached comment by Dr. Byram Bridge:
Fiction Disguised as Science to Promote Hatred
Disinformation Must Be Called Out

Dr. Byram W. Bridle Apr 26
If you only have a few minutes, jump to the section below entitled “Proof that the Paper by Fisman, et al. Should be Retracted Immediately”.
The legacy media has been like pigs at a trough today and yesterday with the publication of an atrocious ‘peer-reviewed’ ‘scientific’ article by Dr. David Fisman, Dr. Ashleigh Tuite, and a graduate student. After all, with raw public health data unable to support the only COVID-19 narrative that has been deemed acceptable, fresh fuel was apparently needed. Lots of media outlets have been reporting on this study; one of them being CTV News. Here is the headline for their article:
“Being with unvaccinated people increases COVID-19 risk for those who are vaccinated: modelling study”
This kind of messaging will only fuel hatred and segregation and the potential development of harmful policies. And it is all in the name of bad science. As a researcher who has published and reviewed many scientific papers, I can tell you that the article by Fisman, et al. is the worst one that I have ever seen. The ‘peer reviewers’ of this article should be ashamed of themselves for allowing this to be published, and the editor even more so. If the Canadian Medical Association Journal does not promptly retract this article, they will have made themselves an embarrassment among scientific publishers.
This paper by Fisman, et al. is only thinly veiled hate speech under the guise of science. Before I walk you through the numerous massive errors in this paper, let me first show you one example of the messaging regarding the impact and relevance of the paper.
Fisman was quoted by CTV News as saying “We thought what was missing from that conversation was, what are the rights of vaccinated people to be protected from unvaccinated people?”. The only reason why Fisman is trying to turn people against other people is due to the abject failure of the COVID-19 ‘vaccines’ to function like vaccines. That is to say that the purpose of a vaccine is to protect people from a pathogen; to prevent both the disease and transmission of the causative agent. Such a medical product does not require one to pit people against people. Fisman has inappropriately labelled critically thinking people as an enemy when the actual culprits are SARS-CoV-2 and overly rushed jabs of exceptionally poor quality and highly questionable safety that have been pushed as the sole solution at the expense of all others.
One of the few accurate statements in the CBC News article was this quote about Fisman where: “he acknowledges that a simple mathematical model doesn’t fully reflect the real world or the diverse factors that must be taken into account when setting public health policy”. This is an understatement if ever I saw one.
I already spend an inordinate amount of time and energy correcting misinformation and disinformation coming from scientists who should know better. As such, I am not going to conduct an exhaustive breakdown of the article by Fisman, et al. However, here are quite a few examples that make it clear that the science is flawed and the messaging not only biased, but completely incorrect…
- Minor issue: “While the ability to vaccinate to herd immunity has been held back by the increasing transmissibility of novel SARS-CoV-2 variants of concern…”. How about considering the fact that the ‘vaccines’ are so far from performing like real vaccines that they never could have been used as tools to achieve herd immunity. The authors of the paper are not immunologists and this has been an ongoing issue when discussions have turned to the immunological sub-discipline of vaccinology. They don’t seem to realize that the term ‘immunity’ in ‘herd immunity’ means protected from disease and transmission of the causative agent of that disease; otherwise herd immunity would be an unrealistic goal. To do this via vaccination, sterilizing or near-sterilizing immunity is required. The current SARS-CoV-2 vaccines don’t come close to meeting this standard. This is painfully obvious by the fact that SARS-CoV-2 has been allowed to become endemic despite most of the population having taken multiple doses. Look at how many work places and other organizations (and cruise ships, and research stations in Antarctica) have had SARS-CoV-2 run rampant through their 100% or almost 100% ‘vaccinated’ populations.
- Major issue: “antivaccine sentiment, fuelled in part by organized disinformation efforts, has resulted in suboptimal uptake of readily available vaccines”.In fact, the article by Fisman, et al. represents one of the most egregious examples of disinformation that I have seen.Most of the people that remain ‘unvaccinated’ are not ‘anti-vaccine’ by any stretch of the imagination. Due to critical thinking and following the science, they are not in support of the current crop of COVID-19 jabs. Remember, the definition of a vaccine was changed to accommodate these jabs. They are nothing like any of the historically mandated vaccines, such as those used in the childhood immunization series.People have been wary because the initial clinical trials to evaluate these ‘vaccines’ are still ongoing, literally meaning the jabs are still in the experimental phase. Other reasons for wariness include that the stated endpoint of the ongoing clinical trials is a reduction in cases of COVID-19, which they are failing to do. Hesitancy is because the placebo control arms of the clinical trials were removed (in contravention of study protocols) after a median follow-up time of only two months so no mid- to long-term safety signals can be detected via active monitoring. It is because the only safety monitoring left is via outdated and flawed passive voluntary monitoring systems that dramatically underestimate adverse events. It is because the vaccines behave in stark contrast to what was publicly stated. For example, they don’t stay at the injection site. Rather, the mRNA vaccines get distributed throughout the body (see my recent article about this). It is because serious side-effects were only unveiled after the rollout into the public, leading to things like the AstraZeneca ‘vaccine’ being deemed too dangerous for Canadian adults (many other countries detected the blood clotting problem and avoided this jab and then had to teach Canadian health authorities about this problem) and the Moderna vaccine being declared too dangerous for young males by harming their hearts.Other reasons for COVID-19 vaccine hesitancy include public health ‘experts’ disseminating disinformation like what is contained in the article by Fisman, et al. Also, many people recognize the validity of naturally acquired immunity and the massive accumulation of literature that shows it is superior in almost every way to the ‘vaccine’-induced immune responses. And there are a myriad of other reasons.I refer to this as a major issue because Fisman and his colleagues are labeling people and using subjective argumentation in an attempt to justify it. This sentence in the paper has no place in the world of objective science.
- Major problem: “Nonvaccination is expected to result in amplification of disease transmission in unvaccinated subpopulations, but the communicable nature of infectious diseases means that this also heightens risk for vaccinated populations”. Some critical considerations have been missed here. The issue is not about nonvaccinated versus vaccinated people; it is about who is immune and who is not. Fisman, et al. really need some advanced immunology training before opining about vaccines. They need to realize that immune responses to vaccination follow a bell-shaped curve in an outbred population like humans. Most people respond moderately well. A few will respond very robustly; these are the high responders. And then a minority will be low- or non-responders. These individuals will have no protection against disease. As such, showing certification of having received two or more jabs does not guarantee immunity. And then there is the reality that the human immune system can work in the absence of external ‘hand of man’ interventions. This means that our immune systems can mount protective responses to natural infections. Having lived with SARS-CoV-2 for more than two years and with the Delta and Omicron variants having ripped through the population, a vast majority of ‘unvaccinated’ people would be expected to have naturally acquired immunity. Conflating the concepts of immunity and vaccination represents a major conceptual flaw with this paper. I recommend that Fisman and his colleagues review this video that I am in full agreement with: Fauci teaches that natural infection is the best form of vaccination.
- Major issue that proved to be a fatal flaw: “We also assumed that some fraction of the unvaccinated population had immunity at baseline owing to previous infection and that a fraction of the population was vaccinated”. Initially, this seems reasonable. But then one learns that the number plugged into the simple mathematical model was only 20% of the population having naturally acquired immunity. Really?!? After more than two years of living with SARS-CoV-2 and and Delta and Omicron sweeping through Canada, one is to believe that only 20% have immunity? Where is the evidence for this? A paper showing that a vast majority of Canadians might have some degree of naturally acquired or cross-reactive immunity against SARS-CoV-2 can be found here. I would expect that even more unvaccinated Canadians would now have natural immunity. Unfortunately, the Canadian taskforce for gathering data about immunity among our population was disbanded so we missed the boat on tracking this incredibly important parameter that would have a major influence on any epidemiological model. So, what is the source of data used by Fisman, et al. to come up with their proposition of 20% immunity with a ‘plausible’ range of 10-50%? The source is stated as “assumption”! Isn’t that interesting. This is notable because all mathematical models are only as good as the assumptions that are plugged into them. The old adage is ‘garbage in, garbage out’. I will show you below how this single unjustified assumption biased the conclusions of the paper.
- Fatal flaw: “We treated immunity after vaccination as an all-or-none phenomenon, with a fraction of vaccinated people (as defined by vaccine effectiveness) entering the model in the immune state and the remainder being left in the susceptible state. For example, a vaccine that is 80% efficacious would result in 80% of vaccinated people becoming immune, with the remaining 20% being susceptible to infection.” There are multiple major issues here. First, the COVID-19 ‘vaccines’ fail to confer immunity, which is protection against disease and transmission. It is common knowledge that ‘vaccinated’ people get infected and sick at least as much as, if not more than the ‘unvaccinated’. This is why a desperate emphasis has been placed on the debatable possibility that disease severity is merely dampened by ‘vaccination’. A such, a biologically incorrect assumption was made here. Also, the effectiveness of the vaccine that was plugged into the model started at 40% and went up from there. However, these high percentages represent relative risk reduction, not absolute risk reduction. Do you remember when we were told that Pfizer’s ‘vaccine’ was 95% effective? That did not mean that 95% of the population was protected against getting COVID-19 (or 80% as used in the example in the paper). That 95% reduction was a relative risk reduction. What many people were not told is that most of the people in Pfizer’s clinical trial never got COVID-19, which is the disease that can occur in some people who get infected with SARS-CoV-2. In fact, the absolute risk reduction at the population level in the study was a mere 0.84% as a result of ‘vaccination’. As such, it is completely inappropriate for Fisman, et al. to plug values for relative risk reduction into their population-level models and treat them as though they represent absolute risk reduction. Conflating relative versus absolute risk reduction was misleading. As expert epidemiologists the authors must surely know the difference between absolute versus relative risk reduction. This is evidence that what they disseminated was disinformation.
- Fatal flaw: “We did not model waning immunity”. I was flabbergasted by this assumption. COVID-19 ‘vaccine’-induced immunity is ridiculously short-lived. In contrast, naturally acquired immunity is much longer-lived. This differential effect would have had a major influence on the outcome of the mathematical model. This assumption by the authors ignores obvious scientific facts.
- Major issue: There was no discussion about assumptions with respect to the safety (or lack thereof) of the COVID-19 ‘vaccines’ that might offset the perceived value of ‘vaccination’. Regardless of their viewpoint, they should have discussed this and provided evidence for their stance.
- Major issue: “Boosting with mRNA vaccines appears to restore vaccine effectiveness at least temporarily against Omicron”. This is not an accurate assumption to make. The paper that was cited to justify this statement used data derived from a simplistic model in a petri dish. It provided evidence of the presence of SARS-CoV-2-neutralizing antibodies in the blood of people who received COVID-19 booster ‘vaccines’. However, this lacked a functional context. First, these antibodies were measured in blood, but the virus infects the airways, so the anatomical location that was studied is irrelevant. Second, it is possible that there were non-neutralizing antibodies that could actually enhance disease but no testing was performed to detect these; non-neutralizing antibodies were ignored. There are other issues, but the point is that there was no way of knowing whether the subset of antibodies measured in the cited study would translate into any degree of protection against ‘real world’ infection. This shows a bias by Fisman, et al. in pushing booster doses with the weakest of data to support it.
- A refreshing truth: “The simplicity of our model is… a weakness, because it does not precisely simulate a real-world pandemic process in all its complexity”. This is an understatement and is one of the reasons why the paper should be retracted.
- Major issue: The paper treats COVID-19 ‘vaccines’ as though these are the only way to reduce the harm of COVID-19 among Canadians. There was no discussion of alternative strategies such as prophylaxis or treatment using re-purposed drugs, the promotion of vitamin D sufficiency (a vital molecule for optimal functioning of the immune system) among a population in a northern climate that is plagued with seasonal vitamin D insufficiency, etc.
- Major issue: Fisman declared the following competing interests: “David Fisman has served on advisory boards related to influenza and SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca and Sanofi-Pasteur Vaccines”! These seem like inappropriate conflicts of interest, especially in light of the major flaws in his paper. In combination, these are suggestive of an inappropriate bias in judgement.
- Minor issue: “He also served as a volunteer scientist on the Ontario COVID-19 Science Advisory Table”. My issue here is not related to a conflict of interest, but rather the shoddy epidemiological modeling in his current paper raises serious questions about all of the historical modeling done with the Ontario Science Table. Journalist Brian Lilley published an article in the Toronto Sun on March 16, 2022 about the poor track record of mathematical modeling by the Ontario Science Table (of which Fisman is a former key member of the modeling group). It included these quotes…“The self-appointed, self-important Science Table has been wrong with their modelling predictions more times, and in more ways, than I can count.”“The Science Table has somehow achieved a revered status in Ontario, a sort of secular sainthood bestowed upon their members and their work despite a spotty track record of predicting how the pandemic is going. They’re not an official government body; in fact, they have no official government role, but they are seen as and presented as the authoritative voice on COVID in the province.”“I’m just judging the Science Table by their track record and if you did that, you wouldn’t be listening to them either.”
- Major issue: The messaging in the paper by Fisman, et al. carries serious implications. It implies that the unvaccinated are selfishly causing harm to the ‘vaccinated’. If the conclusions of the paper were to stand, they would logically lead to things like policies for forced vaccinations or stricter segregation of the ‘unvaccinated’ or harsher penalties against them. It is scary to see scientists using disinformation to promote hatred and division amongst Canadians.
Proof that the Paper by Fisman, et al. Should be Retracted Immediately
For the final ‘nail in the coffin that is the paper by Fisman, et al., let’s make only one adjustment to their model. First, kudos to the authors for making their mathematical model available. Seeing the epidemiological models being used to inform COVID-19 policies has been a rarity over the past couple of years. Fisman did not make his model available in his previous paper (that was also published in the Canadian Medical Association Journal), nor for any models that he was involved with when serving on the Science Table. Unfortunately, the current disclosed model highlights exactly why nobody should ever trust any epidemiological model that has not been fully disclosed. I encourage you to download the model. You can find it as a Microsoft Excel file here.
Now select the first tab, entitled “Patch Model”. In the top left corner of this page you will see “Model Symbology and Parameters”…
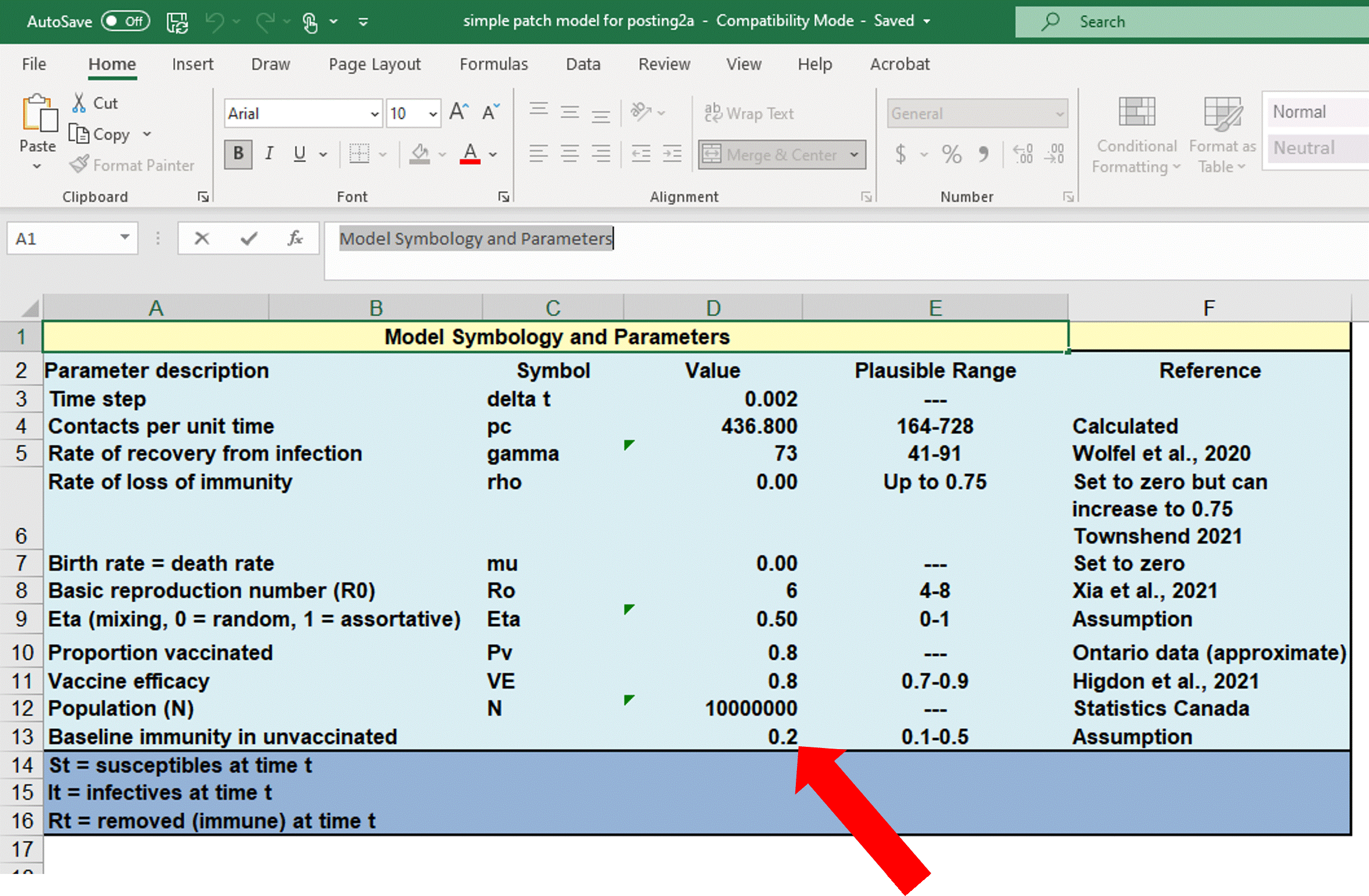
Note that the default value used for baseline immunity among the ‘unvaccinated’ was a mere 20%, which was based on pure speculation (se the ‘Reference’ column, cell F13). Remember, I cited a peer-reviewed published scientific paper suggesting that ~90% have immunity.
If you scroll to the right on the same Excel page, you will find the following data starting at cell AD19…
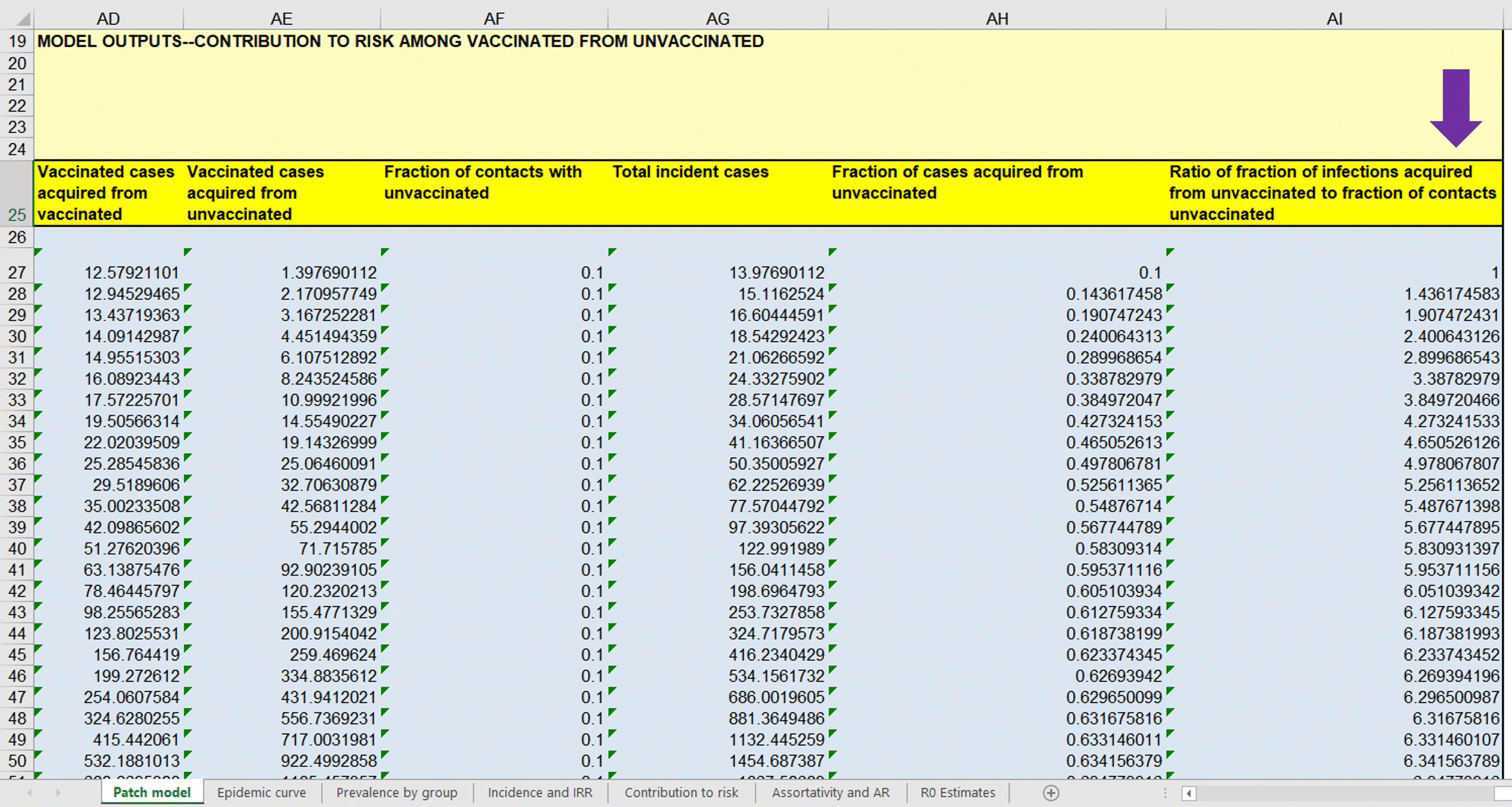
…below the purple arrow are numbers that provide a theoretical indication of the proportion of cases of COVID-19 that ‘vaccinated’ people got from the ‘unvaccinated’ after normalizing for their amount of contact people with the ‘unvaccinated’ group. A number larger than ‘1’ indicates that cases of COVID-19 among the ‘vaccinated’ came disproportionately from contact with the ‘unvaccinated’. The first row of data represents the starting point of a theoretical wave of COVID-19, hence the reason why column AI27 starts at ‘1’. As you move down the column, the time into the modeled wave of cases of COVID-19 increases. Note that the ratios rapidly rise well above ‘1’, suggesting a bias in transmission coming from the ‘unvaccinated’. This is the basis for Fisman, et al. promoting fear of the ‘unvaccinated’.
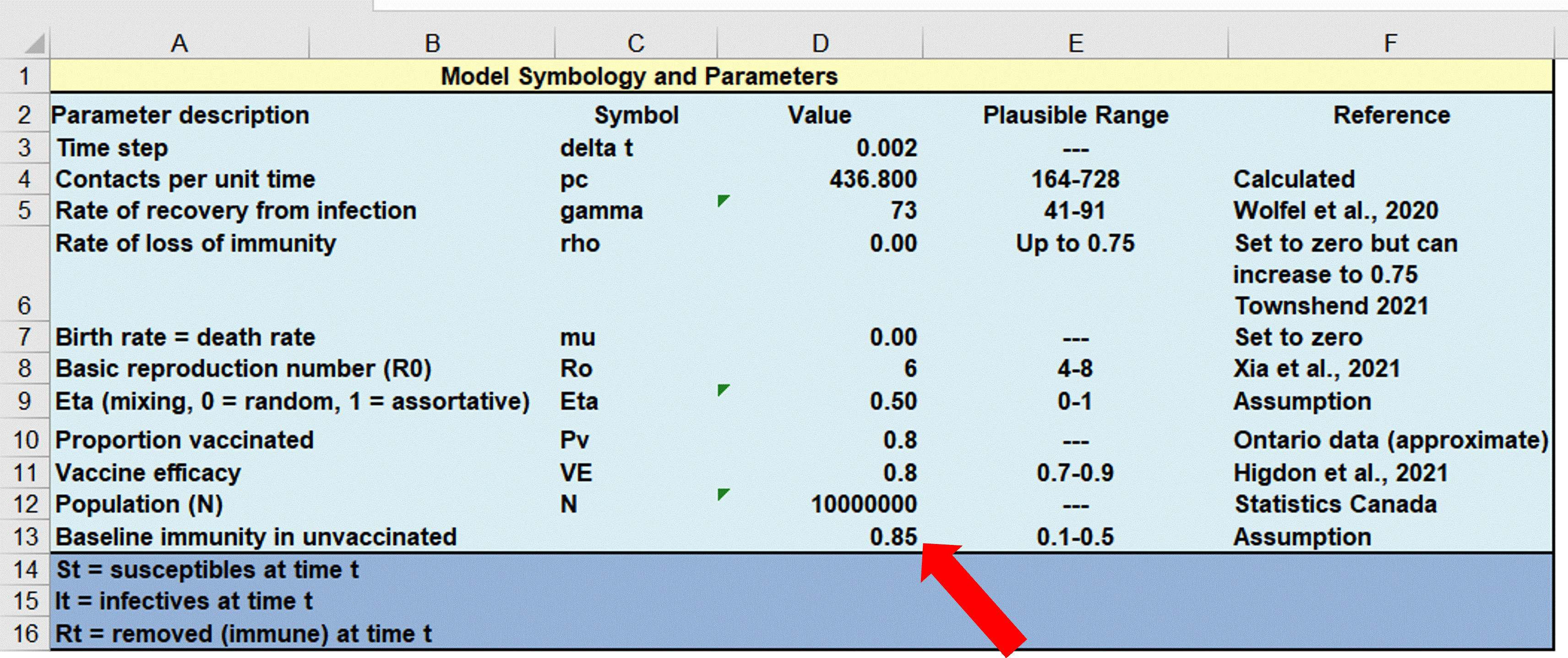
However, I have provided an excellent-quality peer-reviewed scientific article as a reference that suggests that immunity among ‘unvaccinated’ people in British Columbia was ~90%. To be conservative, let’s say it is only ~85% across Canada, despite this likely being an underestimate as most Canadians were exposed during the record-shattering waves caused by the Delta and Omicron variants sweeping through the country. So, let’s change this single parameter in the mathematical model to see what happens. I changed the proportion of the ‘unvaccinated’ with immunity from 20% to a justifiable 85%…
…now look at the effect this had on the data (look under the purple arrow)…
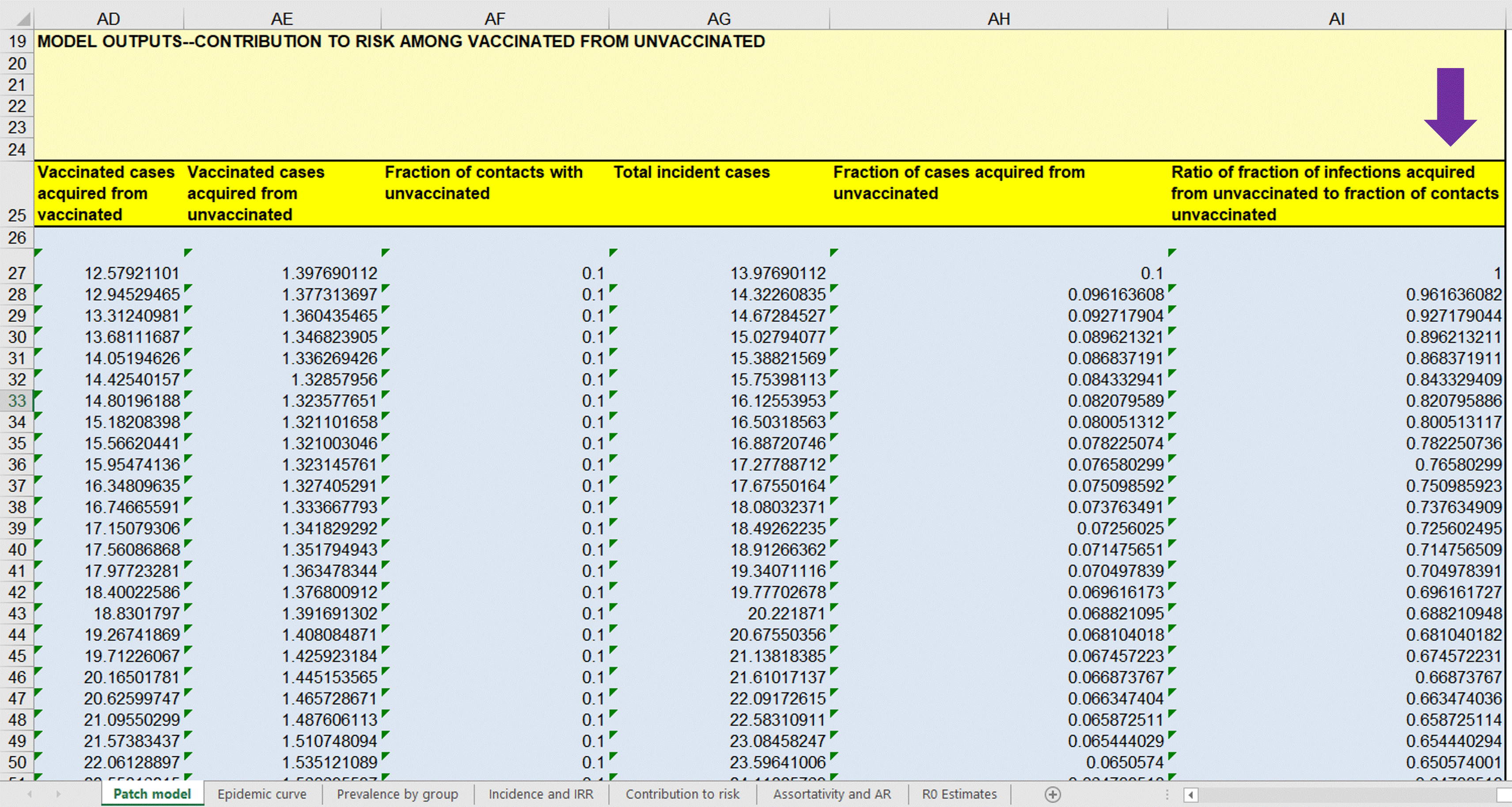
…remarkable, isn’t it! Correcting only this one assumption completely reverses the conclusions of the paper. All of a sudden every ratio drops below ‘1’, meaning that transmission is occurring disproportionately from ‘vaccinated’ people. Now the ‘unvaccinated’ are serving as a protective buffer for the ‘vaccinated’.
Now one must ask how skewed the conclusions of the paper would go in the opposite direction if the several other incorrect assumptions were to be corrected. As you can plainly see, this paper by Fisman, et al. is nothing short of preposterous. How could a paper be allowed to be published in what used to be a respected medical journal when its conclusions get completely reversed when only one of several reasonable corrections are made! The paper by Fisman, et al. is a classic demonstration of ‘garbage in, garbage out’. The authors are very intelligent, well-trained scientists who ply their trade well. They know what they are doing. As such, in my expert opinion, their paper represents disinformation (i.e., the deliberate dissemination of misinformation). I would be willing to stand in a court to justify my opinion. I honestly believe that the authors need to be investigated, as does the editor who allowed the paper to be published; and it would be great if the names of the reviewers who supported its publication could be made public. And the legacy media outlets that are promoting this ‘scientific’ garbage should be ashamed. They could use some immunology expertise and a return to investigative journalism to separate themselves from being labeled as propaganda artists.
Modeling Should Predict ‘Real World’ Data
Here are some ‘real world’ data that Fisman, et al. would be wise to consider in their modeling. This was copied from the website of the Ontario Ministry of health on April 26, 2022…
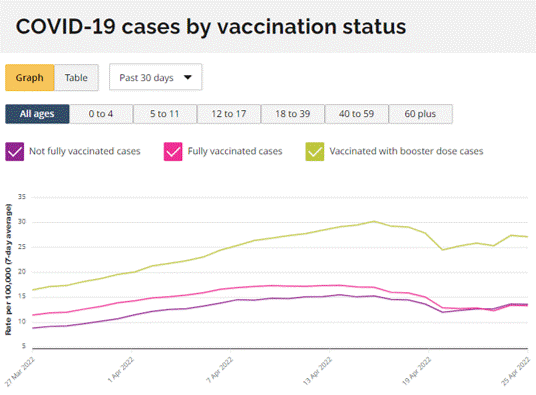
At the end of their paper, Fisman, et al. strongly promoted booster doses as a way to reduce ‘infections’. Yet the ‘real world’ data clearly show that the boosted sub-population is being diagnosed with disproportionately more cases than the ‘not fully vaccinated’ group, which includes the ‘unvaccinated’ and people who received a single dose. Why would someone want to take a booster and more than double their risk of getting diagnosed with COVID-19?!? Which is stronger evidence, the public health data shown above or contradictory messaging based on inappropriate massaging of a purely theoretical model? When mathematical models are misused they become no more utilitarian than toys.
A Direct Message to Fisman, et al.
Fisman and Tuite: Your paper, which can be flipped on its head by correcting just one of your multiple incorrect immunological assumptions, stigmatizes the ‘unvaccinated’ and could potentially be used to justify policies as draconian as forced inoculations. Why are you even promoting messaging based on theoretical models using assumptions that you are not qualified to opine on when concrete scientific evidence about transmission could be generated via biological sampling? You owe Canadians an apology for disseminating harmful disinformation. Should you wish to contest my immunological critiques, I would invite you to arrange a forum where we can have an objective third party moderate a respectful discussion about COVID-19 vaccinology in front of the Canadian public with equal representatives on both sides of the debate.
A Message to the Administration of the University of Toronto
You should launch an investigation into the academic conduct of Drs. Fisman and Tuite.
A Message to the College of Physicians and Surgeons of Canada
You should investigate Dr. Fisman and the harms that may be caused by his actions as a physician in publishing a misleading scientific paper in a medical journal.
A Message to the Canadian Medical Association Journal
Do the right thing and immediately retract the paper by Fisman, et al. There is a rumour that you may have sent this paper directly to Canadian physicians. If true, make it very clear to them that the paper represented disinformation disseminated by a physician who knows better. You should reconsider future recruitment of the services of the reviewers that promoted the publication of this paper and recommend that their academic institutions review their conduct. You should also review the conduct of your editorial board and peer review process.
A Message to the Legacy Media
Make the right choice and do everything that you can to blunt the profound harms caused by your rampant and widespread dissemination of misinformation. It is promoting hatred against critically thinking people who made highly informed and justified choices to avoid inoculations that are still in their initial clinical experimentation phase and for about which there is profound scientific debate. Protect the people that you have inappropriately placed at risk. You know where it will lead if you promote polarization of two groups of people and fuel feelings of anger and hatred in one of them against the other. Replace journalists with those who are willing to think critically and who will not support censorship of legitimate experts with ‘dissenting’ views. Nor should peer-reviewed scientific papers be treated like the gospel truth. The anonymous peer review process is fallible.
A Message to All Canadians
We are more alike than different. Do not fall into the trap set in the paper by Fisman, et al. to equate ‘likeness’ with ‘vaccination’ status. As an expert vaccinologist who has been closely following the accumulating science and, more importantly, as a fellow human being, I implore you to promote unity.
Correcting the Disinformation
Fisman had Tweeted, “Our paper supports the idea that the decision to remain unvaccinated confers risk not only on the unvaccinated individual but (disproportionate to contact rates) on vaccinated individuals too”.
If Fisman were to demonstrate objectivity as a scientist, he would update his Tweet to state something like the following: “After correcting just one of the several inappropriate immunological assumptions, our paper now supports the idea that the decision to get ‘vaccinated’ confers risk not only on the ‘vaccinated’ individual but (disproportionate to contact rates) on ‘unvaccinated’ individuals too; unlike our previous conclusion, this corrected model matches real-world data. Thank-you to those who chose to remained ‘unvaccinated’ since you are now selflessly serving as a buffer to the ‘vaccinated’. We are sorry to the field of public health modeling for disclosing how easy it is for the conclusions of our models to be manipulated by assumptions that we sometimes pull out of thin air. We also apologize to ‘unvaccinated’ people (most of whom have received legitimate vaccines throughout their lifetimes) for misleading media organizations around the world into promoting hatred against you. Now that our model has been shown to point to the ‘vaccinated’ as the main culprits of transmission of SARS-CoV-2, we implore you to not promote hatred against us like we have done to you.”
…don’t worry Dr. Fisman, I can tell you sincerely and from experience that the vast majority of ‘unvaccinated’ people will not return ill wishes in kind, even as more hypocritical messaging is unveiled. I for one want to see unity restored among Canadians. Hatred, segregation, and mislabeling of people have no place here. Much healing needs to happen and your current misdeed has been very counterproductive.
Overall Conclusions
No government should be allowed to implement policies based on results of epidemiological modeling prior to full disclosure of the data, the model used to generate predictions, and the conflicts of interests of the modelers. As demonstrated by Fisman, et al., public health models in the hands of the wrong people can result in devastatingly harmful and brutally misleading public messaging. This, in turn, could lead to the introduction of inappropriate health policies. And finally, multiple objective immunologists should always be consulted to advise on the immunological parameters being plugged into any health-related models.
In the name of good science, the correction of mis/dis-information, and in a desperate attempt to maintain some public faith in vaccinology,
Byram
Dispelling the Myth of the Unvaccinated